Cancer of Nasopharynx
Head and Neck Tumour Surgery
Cancer of Nasopharynx
Where is Nasopharynx?
The nasopharynx is the air passageway at the upper part of the pharynx (throat) behind the nose and lies just above the soft palate (Fig.1 Coloured pink). The nostrils lead through the nasal cavity into the nasopharynx. An opening on each side of the nasopharynx (called the Eustachian tube opening) leads into the middle ear on each side. Inferiorly, it communicates with the oropharynx (part of pharynx behind the oral cavity).
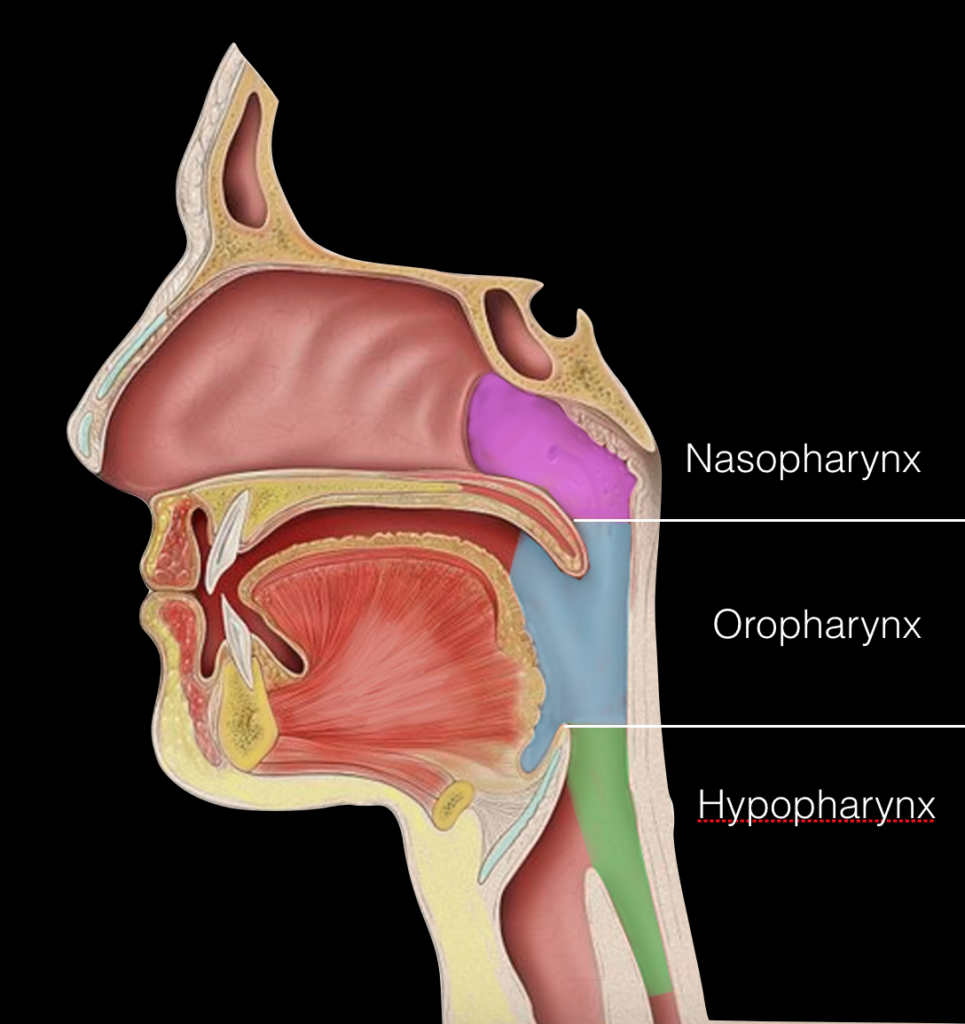
Fig.1
What type of tumours develop in nasopharynx?
Several types of tumours can develop in the nasopharynx. Some of these tumours are benign (non-cancerous), but others are malignant (cancerous). Several types of benign tumours, including angiofibromas, hemangiomas etc.
The nasopharynx contains several types of tissue, and each contains several types of cells. Different cancers can develop in each kind of cell. The differences are important because they determine the seriousness of the cancer and the type of treatment needed. Squamous cell carcinoma (nasopharyngeal carcinoma – NPC) is the most common malignant tumour of the nasopharynx. Other nasopharyngeal cancers include adenoid cystic and mucoepidermoid carcinomas, malignant mixed tumours, adenocarcinomas, lymphomas, fibrosarcomas, osteosarcomas, chondrosarcomas, and melanomas.
Who does it affect?
NPC is one of the most common cancers among people of Chinese, especially Southern Chinese, and Southeast Asian ancestry, including Chinese immigrants to North America. Over several generations, the prevalence among Chinese-Americans gradually decreases to that among non-Chinese Americans, suggesting an environmental component to etiology. Dietary exposure to nitrites and salted fish also is thought to increase risk. Epstein-Barr virus is a significant risk factor, and there is hereditary predisposition.
What symptoms does it cause?
- Nasal obstruction
- Hearing loss due to a middle ear effusion (eustachian tube obstruction)
- Purulent bloody nasal discharge
- Frank epistaxis
- Cervical lymphadenopathy
- Pain in the side of the head (due to involvement of fifth cranial nerve)
- Blurred or double vision (3rd, 4th, and 6th cranial nerve palsies)
- These symptoms may be caused by other conditions also. Therefore, there is always a big delay between the onset of symptoms and final diagnosis. As a result, most patients usually present at late stages.
How is it diagnosed?
Anyone with such symptoms requires careful evaluation and examination with a nasopharyngeal mirror or endoscope, and lesions are biopsied. Open cervical node biopsy should not be done as the initial procedure, although a needle biopsy is acceptable and often recommended. Gadolinium-enhanced MRI (with fat suppression) of the head with attention to the nasopharynx and skull base is done; the skull base is involved in about 25% of patients. CT also is required to accurately assess skull base bony changes, which are less visible on MRI. A PET scan also commonly is done to assess the extent of disease as well as the cervical lymphatics.
How is it treated?
Primary treatment of NPC is concomitant chemoradiotherapy, in which chemotherapy is given in combination with radiation therapy. Patients achieve quite satisfactory cure rate. About one third of the patients fail locally in the nasopharynx. Up until recently there were no good treatment options available other than re-irradiation.
Re-irradiation improves survival in less than 30% of patients but associated with high incidence of complications (of reirradiation) like temporal lobe necrosis, trismus, deafness, endocrine dysfunction and osteoradionecrosis causing severe pain, foul odour and massive bleeding. Even though the incidence of complications has come down with intensity modulated radiotherapy (IMRT), the cure rate remains the same.
Surgery improves survival in more than 50% in these lesions with minimal morbidity. Today’s evidence favours surgery in these recurrent or residual tumours.
Surgery
Prof. Rayappa is a pioneer in open as well as endoscopic surgery for malignant nasopharyngeal tumours in this country.
Removing the tumour (Nasopharyngectomy)
For long, nasopharynx was considered unresectable because of its central location and was surrounded by uninvolved bony structures. Access to the nasopharynx has been pioneered by many surgeons in the last three decades using various open techniques e.g.,. Trans temporal approach by UgoFischin 1983. William Wei in 1989 translocated the upper jaw bone (facial translocation or maxillary swing VIDEO) to expose this region well for an en-bloc resection.
Paul Donald described the Transfacial Subcranial approach for nasopharyngectomy. This has doubled the 5-year survival in patients with recurrent disease.
With newer endoscopic surgical techniques, surgeons can completely remove some nasopharyngeal tumours (endoscopic nasopharyngectomy), but this is appropriate only for a small tumours. Factors determining the surgical approach are the extent of tumourand the structures involved. For planning the surgery, we should know whether the tumour is limited to nasopharynx or spread to infratemporal fossa or involving the internal carotid artery or intracranial extension.
Nasopharyngectomy is indicated as a salvage procedure in persistent or recurrent nasopharyngeal carcinoma. But it is done as a primary treatment in radioresistent tumours like adenocarcinomas, minor salivary gland tumours and sarcomas. These complex procedures are done only in specialized centers.
Removing lymph nodes
Cancers of the nasopharynx often spread to the lymph nodes in the neck. These cancers often respond well to treatment with radiation therapy (and sometimes chemotherapy). But if some cancer remains after these treatments, an operation called a neck dissection may be needed to remove these lymph nodes.
Questions patients should ask before deciding about the treatment:
- What type of nasopharyngeal cancer do I have?
- What is the stage of the cancer? What does this mean?
- What are the treatment options?
- What treatment option do you recommend?
- Should I get an additional consultation or second opinion?
- What can be done to relieve the possible side effects?
- If surgery is needed, will it be necessary to have reconstruction done to replace lost tissue ?
- If surgery is needed, will there be a need for a neck dissection (removing lymph nodes)? If so, what type of dissection will be done? What does this mean?
- When can I expect to recover from the treatment effects?
- What follow-up tests will be needed, and how often will I need them?
- Will there be any lasting or late side effects that will need special care?
The Heart Of Clinic

Dr. C. Rayappa MBBS, DLO, FRCS(Edin)
SENIOR CONSULTANT
+91 44 3315 1105
Dr. C. Rayappa graduated from Madras Medical College, Chennai, India in 1982. He completed his post graduation in Otolaryngology (ENT)
For Doctors
Need more information?
Reach us through mail or phone
The Heart Of Clinic
Dr. C. Rayappa MBBS, DLO, FRCS(Edin)
SENIOR CONSULTANT
+91 44 3315 1105
Dr. C. Rayappa graduated from Madras Medical College, Chennai, India in 1982. He completed his post graduation in Otolaryngology (ENT)