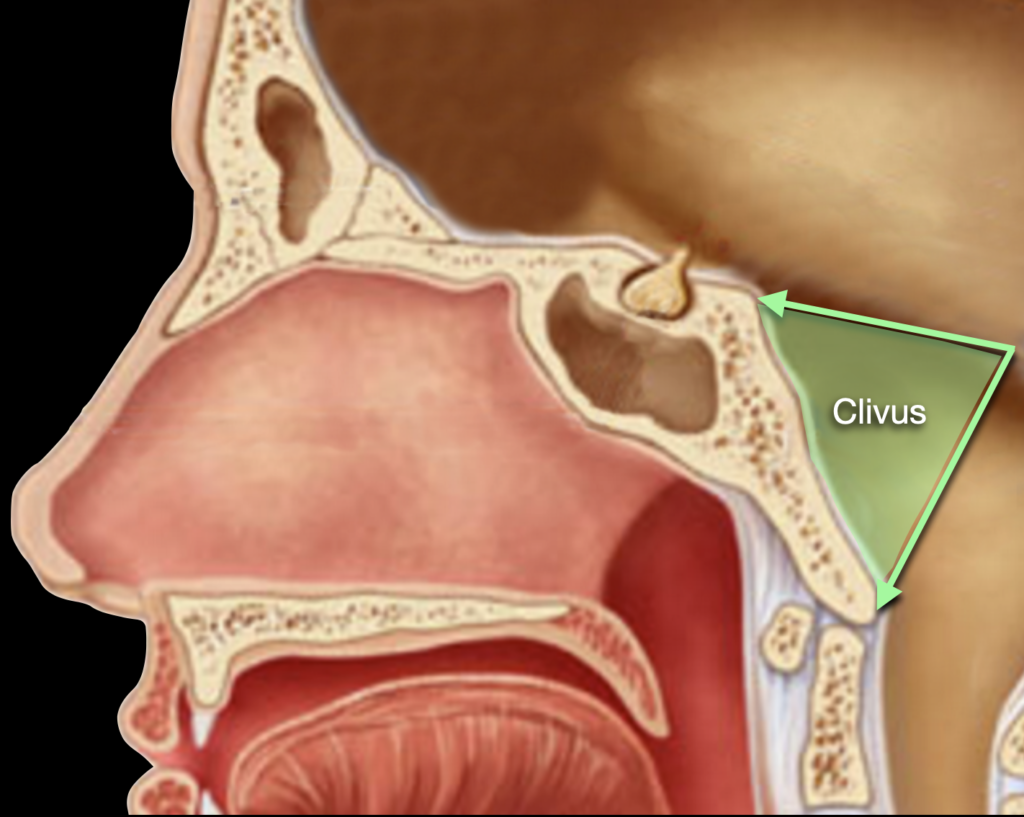
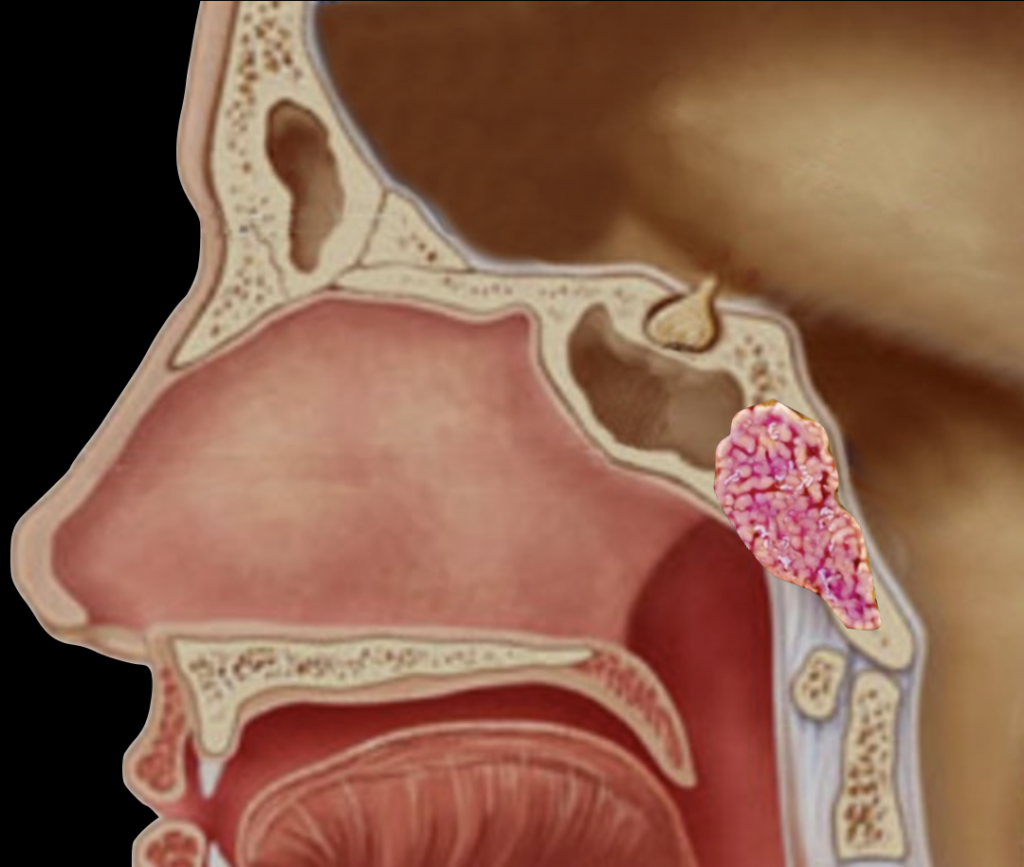
Chordomas are rare, slowly growing malignant tumours originating from embryonic remnants of the primitive notochord which is a flexible rod-like structure present in the human embryo from which the spinal column develops. The notochord usually disappears almost entirely shortly after birth, the cells that give origin to chordoma are left over notochordal cells. It may affect the axial skeleton anywhere from the coccyx to the base of the skull, in either the midline or paramedian position. At the skull base it involves a bone called clivus (Fig.1a & b) which is behind the back of the throat but in front of the brainstem. These are called clival chordomas.
There are three histological subtypes of chordoma: conventional (sometimes called classic), chondroid, and dedifferentiated. Chondroid chordomas tend to be less aggressive than conventional chordomas, while dedifferentiated chordomas are more aggressive, faster growing and more likely to metastasize.
Chordomas of the skull base are particularly debilitating due to the involvement of local structures. The most common signs of chordoma are pain and neurological changes. Most often cause headache, double vision, or gait disturbance.
Currently, surgery is the first-line treatment for chordomas. Complete resection during the first surgery provides the best chances for local control and long-term survival. Using the endoscopic endonasal technique most of these tumours can removed without opening the skull. In addition, larger tumours can be debulked in preparation for radiation therapy with minimal morbidity and rapid recovery time. Surgical goals involve a complete a removal of the grossly identified tumour as possible. Radiation therapy is generally recommended after surgery to kill any remaining tumour cells. Combining maximal surgical resection with high-dose proton radiation therapy is reported to be currently the best management of patients with clival chordoma.
Chordomas are malignant and potentially life threatening tumours. Advances in surgery, radiation and imaging techniques in the past two decades have increased survival rates and improved chances of a cure.
The overall survival rates are 68% at 5 years and 40% at 10 years. Complete surgical resection offers the best chance for long-term survival. In many cases, radiation therapy can also increase local control rates and prolong survival.
Even after surgery and/or radiation, chordomas tend to return locally – in the same location or in the areas around the original tumour. Many patients undergo multiple surgeries over several years to treat local recurrences. Distant metastasis (spreading to other body parts) occurs in 20-40% of patients with chordomas of the spine and less than 10% of patients with skull-base tumours. The most common sites of distant metastasis are the lungs, liver, bones, and skin.