Thyroid Cancer
Head and Neck Tumour Surgery
Thyroid Cancer
Location of thyroid gland and its function
Thyroid gland is a butterfly-shaped gland that lies over the wind pipe (trachea) (Fig.1)that carries air to lungs. It produces a hormone known as thyroxin which helps to regulate body’s metabolism. Behind the thyroid gland, there are four small glands known as parathyroid glands(Fig.2). These secrete a hormone known as parathormone that controls calcium level in the body.
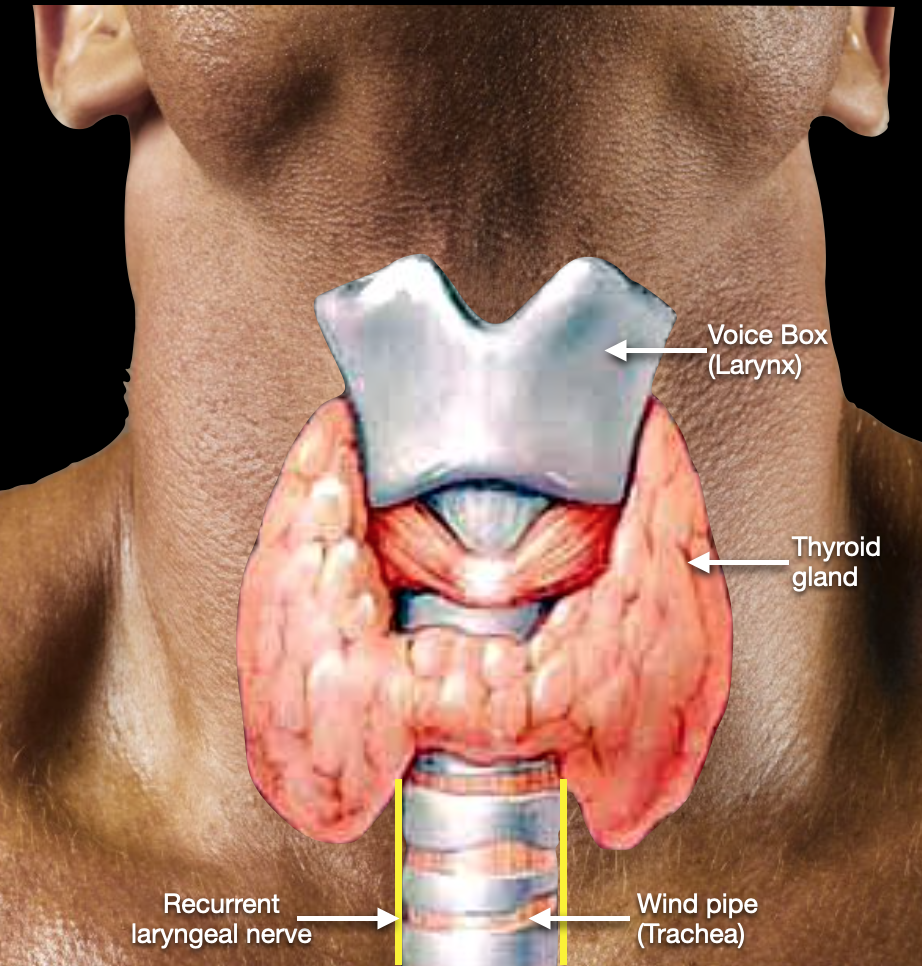
Fig.1
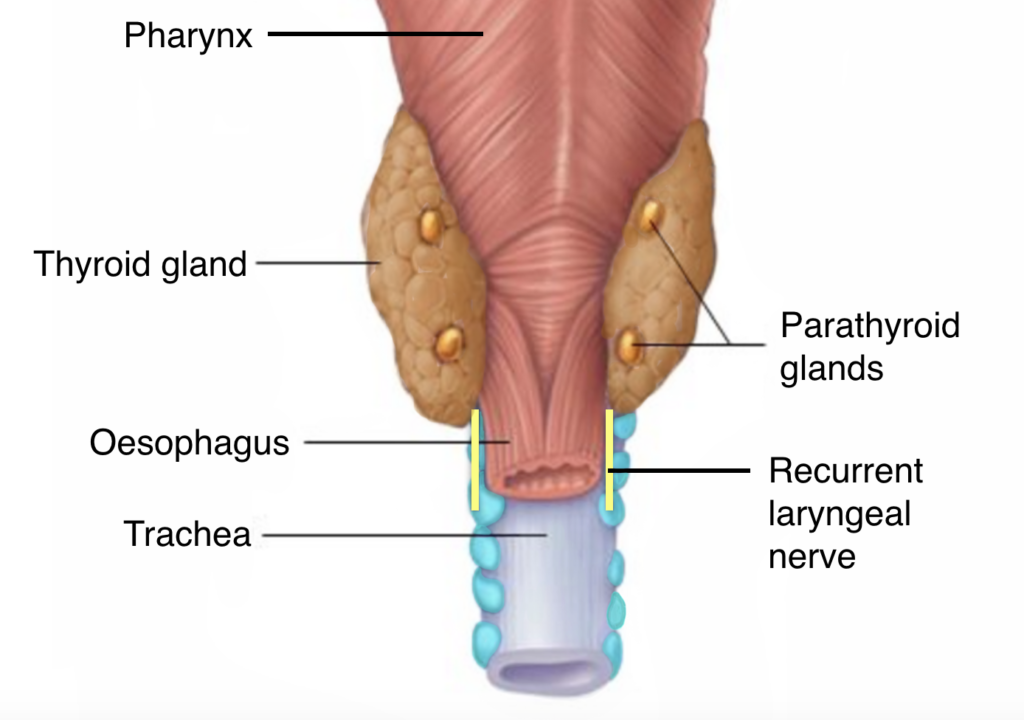
Fig.2.
What type of tumours develop in thyroid gland?
Thyroid tumour begins when cells in the thyroid gland begin to change and grow uncontrollably, forming a nodule (tumour). Ninety percent of all thyroid nodules are benign (noncancerous), but a few are malignant (cancerous). Malignancy should be suspected when there is a prior history of radiation, rapid growth of the nodules, males, extremes of age (less than15 yrs or more than 45 yrs), family history of thyroid cancer, associated with difficulty in swallowing and change in voice.
It is one of the most curable types of cancer — approximately 95 percent of people with a thyroid tumour survive at least five years beyond their diagnosis. Ultrasound done by an expert sonologist is the investigation of choice. Tissue sample is aspirated using small bore needle and send for pathological examination (FNAC). It helps in reaching a diagnosis and plan treatment.
There are different types of thyroid cancers:
Papillary Carcinoma
The majority of all thyroid cancers are papillary carcinoma, a slow-growing tumour. They can spread to the lymph nodes in the neck. Most people with this type of cancer can be cured.
Follicular Carcinoma
This slow-growing thyroid cancer is less common and can often be cured. Follicular carcinoma rarely spreads to the lymph nodes, although it can spread to other parts of the body, such as the lungs and bones.
Hurthle Cell Carcinoma
Hurthle cell carcinoma is a rare type of follicular carcinoma. They absorb less radioactive iodine than papillary and follicular thyroid tumours and therefore surgery is the only treatment.
Medullary Thyroid Carcinoma (MTC)
This rare type of thyroid cancer begins in the C cells, which make the hormone calcitonin. High levels of calcitonin and a protein called carcinoembryonic antigen (CEA) are a common indication of MTC. MTC usually occurs in older adults and often affects only one lobe of the thyroid. Some patients have familial MTC, an inherited form of thyroid cancer that develops during childhood or early adulthood and in several areas of each lobe. These tend to spread to large numbers of lymph nodes very early on, and therefore require a much more aggressive operation than the more localized thyroid cancers, such as papillary and follicular thyroid cancer.
Anaplastic Carcinoma
Anaplastic carcinoma, also called undifferentiated carcinoma, usually develops from an existing papillary or follicular carcinoma. This aggressive type of cancer, which spreads rapidly throughout the neck and to other parts of the body, is very difficult to control.
What symptoms does it cause?
Many patients with thyroid cancer have no symptoms. When they do occur, the first symptom is often a swelling or a small nodule (lump) on the front of the neck. Thyroid nodules are common and are usually painless. The vast majority of them are benign. Other less common symptoms of thyroid cancer are hoarseness of voice, difficulty in swallowing, swollen glands in the neck and difficulty in breathing.
How is it treated?
Once an accurate diagnosis is made, your doctor may recommend any of several treatment options, depending on the type, size, and extent of the tumor, and your general health.
Surgery
Surgery is the main treatment. Both papillary and follicular thyroid cancers are typically treated with complete removal of the lobe of the thyroid that harbors the cancer, in addition to the removal of all of the other side. Surgeon will take sufficient care to safeguard the recurrent laryngeal nerve (nerve that controls the movement of vocal cord) as well as parathyroid glands while removing the thyroid gland(Fig.3). Medullary carcinoma tend to spread to large numbers of lymph nodes very early on, and therefore require a much more aggressive operation than the more localized thyroid cancers, such as papillary and follicular thyroid cancer.
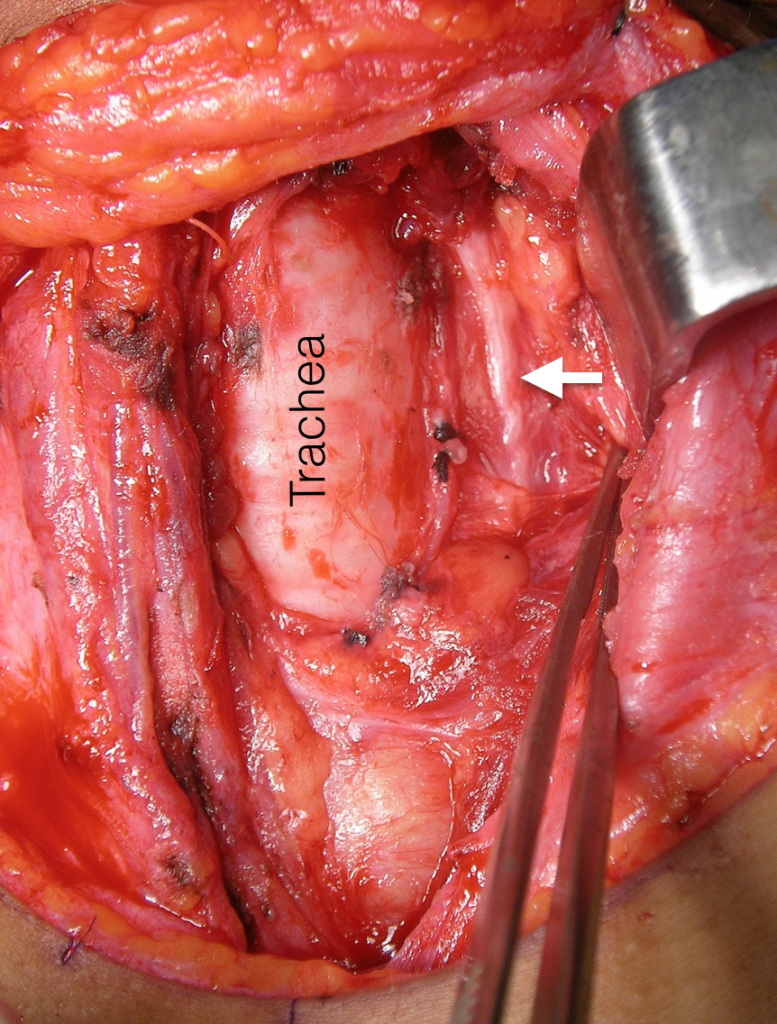
Fig.3. After removal of left lobe of thyroid. White arrow points at the recurrent laryngeal nerve in tracheo-oesophageal groove
Sometimes the tumours are extensive when the patient seeks advice and the tumour is found invading the trachea (wind pipe). In these patients, the segment of trachea invaded by the tumour is resected safely along with the thyroid. After that, the cut ends of trachea are sutured together. Basically, surgery would involve resecting the structures involved by the tumour like windpipe and food pipe and then reconstructing the food pipe and windpipe. Removal of the lymph nodes in the neck, also called lymph node dissection, may be required if the tumour has spread or is at risk of spreading to the lymph nodes.
Radioactive Iodine Therapy
Thyroid cells are unique among all cells of the human body. They are the only cells that have the ability to absorb iodine. Iodine is required for thyroid cells to produce thyroid hormone, so they absorb it out of the bloodstream and concentrate it inside the cell. Most thyroid cancer cells retain this ability to absorb and concentrate iodine. This provides a perfect treatment strategy.
Radioactive Iodine is given to the patient with thyroid cancer after their cancer has been removed. If there are any normal thyroid cells or any remaining thyroid cancer cells in the patient’s body, then these cells will absorb and concentrate the radioactive iodine. Since all other cells of our bodies cannot absorb the radioactive iodine, they are unharmed. The thyroid cancer cells, however, will concentrate the radioactive iodine within themselves and the radioactivity destroys the cell from within without causing sickness, hair loss, nausea, diarrhoea, or pain.
Patients with medullary thyroid cancer and anaplastic cancer usually do not need iodine therapy because these cancers almost never absorb the radioactive iodine. Thyroid stimulating hormone (TSH), produced by the pituitary gland, helps thyroid tissue absorb iodine. However, thyroid hormone therapy can reduce TSH levels and decrease the effectiveness of RAI therapy. Patients are required to stop taking thyroid replacement pills for a period of 4 weeks prior to RAI therapy to increase TSH production. This results in hypothyroidism (low thyroid hormone), which causes a variety of symptoms such as fatigue, depression, weight gain, constipation, muscle aches, and reduced concentration.
Now, we have an alternative method of raising TSH levels. A recombinant TSH may be given at the beginning of RAI therapy to raise TSH levels without having to stop taking thyroid replacement medication.
Thyroid Hormone Therapy
Thyroid hormone is essential for normal function of human body. After removal of thyroid gland, the thyroid hormone needs to be replaced in a tablet form. Thyroid hormone therapy also helps to combat the recurrence of thyroid cancer by suppressing the Thyroid-stimulating hormone (which can stimulate the growth of cancer cells) produced by the pituitary gland. Therefore, patients are advised to take thyroid hormone pills after surgery.
Thyroid cancer is a unique cancer which has good survival even if the disease has spread to other parts of the body. Main stay of treatment is surgery. Radioactive iodine therapy (RAI) destroys remnant thyroid tissue and is also used to treat the tumour cells that have spread to other parts of body. Thus, RAI is beneficial in the post-operative management of high risk differentiated thyroid carcinoma.
The Heart Of Clinic

Dr. C. Rayappa MBBS, DLO, FRCS(Edin)
SENIOR CONSULTANT
+91 44 3315 1105
Dr. C. Rayappa graduated from Madras Medical College, Chennai, India in 1982. He completed his post graduation in Otolaryngology (ENT)
For Doctors
Need more information?
Reach us through mail or phone
The Heart Of Clinic
Dr. C. Rayappa MBBS, DLO, FRCS(Edin)
SENIOR CONSULTANT
+91 44 3315 1105
Dr. C. Rayappa graduated from Madras Medical College, Chennai, India in 1982. He completed his post graduation in Otolaryngology (ENT)