Cancer of Oral Cancer
Head and Neck Tumour Surgery
Oral Cancer
Oral cancer is the sixth most common cancer in the world. It accounts for more than 3, 00,000 new cas-es and 1, 45,000 deaths registered annually. India accounts for one-fourth of all oral cancers world-wide. It is the most common cancer in males in India.
More than half of these patients die of the disease, because they present late. By contrast, early diag-nosis and treatment is associated with a good outcome. Late detection makes more radical treatment necessary, leading to increased morbidity associated with loss of function, aesthetics and psychologi-cal problems. Since oral cancers are readily detectable and identifiable at an early stage it should be possible to improve detection and hence the prognosis.
What are the structures in Oral cavity?
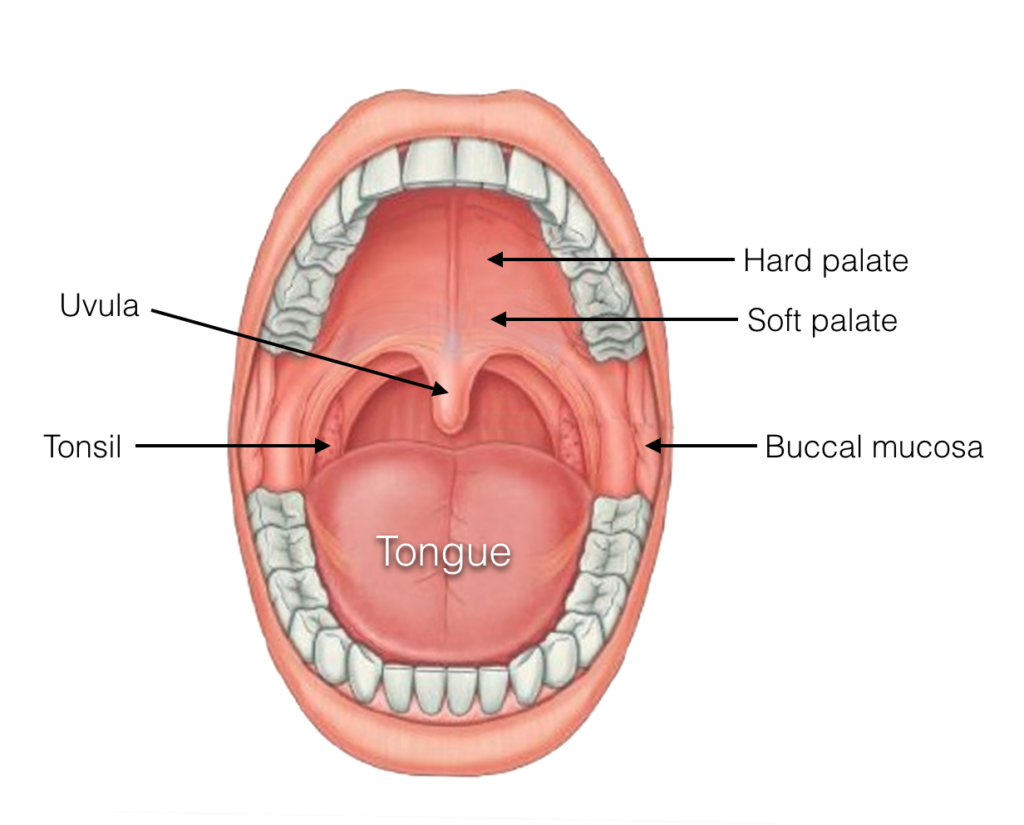
Fig.1
Oral cavity
Oral cavity (Fig.1) includes:
- Lips
- Front two-thirds of the tongue
- Upper and lower gums (the gingiva)
- Lining of the inside of the cheeks and lips (the buccal mucosa)
- Floor of the mouth (under the tongue)
- Hard palate
- Small area behind the wisdom teeth (retromolar trigone)
Oral cavity is made up of many types of cells. When cells divide in an abnormal, uncontrolled way, they can form a non-cancerous (Benign) or cancerous (Malignant) tumours. Oral cancer typically spreads through the lymphatic system to the lymph nodes in the neck.
What are the causes of oral cancer?
Although the aetiology of oral cancer is complex, most Western studies have implicated tobacco smok-ing and alcohol drinking as the major cause of this disease. But in South Asia, in addition to the above factors, chewing of tobacco, betel nut and “pan masala” seems to be the main cause of this problem. Repeated trauma from a sharp tooth or ill-fitting denture may promote neoplastic change over a long period of time.
While the majority of oral cancers arise from a clinically normal mucosal lining, some oral cancers are preceded by pre-malignant changes. They may appear as white patches (Leukoplakia) (Fig.2) or red patches (Erythroplakia) (Fig.3). These may be caused by chronic trauma from sharp tooth or ill-fitting dentures or chemical irritants (tobacco, betel nut etc).

Fig.2 Leukoplakia

Fig.3 Erythroplakia
Another condition very common among Indians is known as sub mucous fibrosis (Fig.4). This is caused by chronic irritation from tobacco juice and pan masala. The lining of whole of mouth and throat are exposed to this irritation, resulting in fibrosis (scarring) underneath the mucosa. The mouth looks pale and the mouth slowly closes due to scar contracture. They are unable to open the mouth, always have a burning sensation in the mouth and have a tendency to develop cancer in multiple areas. Response to radiation therapy is also poor because of poor blood supply in the scarred areas.

Fig.4. Submucous fibrosis
What symptoms does it cause?
- Patients may have one or more of the following symptoms:
- Non-healing ulcer, painless/painful (Fig.5)

Fig.5. Tongue cancer
- Swellings in the gums, palate, tongue etc. (Fig.6)

Fig.6. Cancer of gum
- Loose teeth
- Inability to wear the denture properly
- Difficulty in chewing or swallowing
- Blood in spit
- Lumps in the neck
- Pain in the ear
- A white patch (Leukoplakia) or a red patch (Erythroplakia)
If a patient has any of these symptoms for more than 2 weeks, they should see a doctor. Pain is not an early symptom. A tiny spot, ulcer or small lump should not be ignored, especially if a person is a smoker or drinker.
How is it diagnosed?
After complete clinical examination, the doctor may recommend CT scan or MRI scan or an endoscopic procedure to know the extent of the growth and the structures it is involving. PET scan is done not only to know about the locoregional disease but also to find out whether the disease has spread to other parts of the body.
Incisional or punch biopsies are done under local or general anaesthesia. Fine Needle Aspiration Cytology (FNAC) of the enlarged gland in the neck is done rather than open biopsy to know whether the tumour has spread to the glands.
Also known as mouth cancer, oral cancer typically starts as an ulcer or patch in the mouth
How is it treated?
Nearly half of all head and neck cancers are found in the mouth and throat. Treatment for head and neck cancers may change the way person looks, breathes, talks, eats or swal-lows. Therefore multidisciplinary team approach to patient care is so important. The team includes:
- ENT – Head and neck surgeon
- Plastic Surgeon
- Radiation Oncologist
- Medical Oncologist
- Prosthodontist
- Swallowing Therapist
- Dietician
The treatment options are surgery, radiation therapy and chemotherapy either alone or in combination depending on the stage of tumour. In choosing a treatment plan, factors to consider include overall physical health, the type and stage of cancer, the probability of curing the disease, and the impact of treatment on functions like speech, chewing and swallowing. Surgery or radiotherapy or both modalities combined is usually the most ap-propriate treatment form for curative intent. Chemotherapy is mostly reserved for patients with very advanced cancers.
If the patient undergoes surgery for oral cancer, the surgeon may remove the cancer and some of the healthy, adjoining tissue. Complete surgical clearance of the tumour is achieved with the help of the pathologist who examines the removed tissue at the time of surgery itself (Frozen Section) and says whether the removal was complete or needs fur-ther removal.

Fig.7. Rim resection of mandible. Only the shaded upper half of bone bearing teeth is re-moved. No need to reconstruct the bone.
Small tumours of the oral cavity can be quickly and successfully treated by surgical exci-sion, leaving behind little cosmetic or functional change (Fig.7). Among the advantages for treating early stage cancer with surgery is that it is completed quickly usually requiring a few days of hospital care, instead of 6 weeks of daily Radiotherapy. Dryness of mouth and radiation induced damage to teeth can be avoided. Most importantly, if the patient subsequently develops another cancer in the mouth, throat or voice box, radiotherapy would still be available as treatment option. This will avoid a more significant and disfigur-ing operation. When the index of suspicion is high that there may be cancer cells present in the lymph nodes, an operation called a neck dissection is performed.
Reconstruction of lower jaw
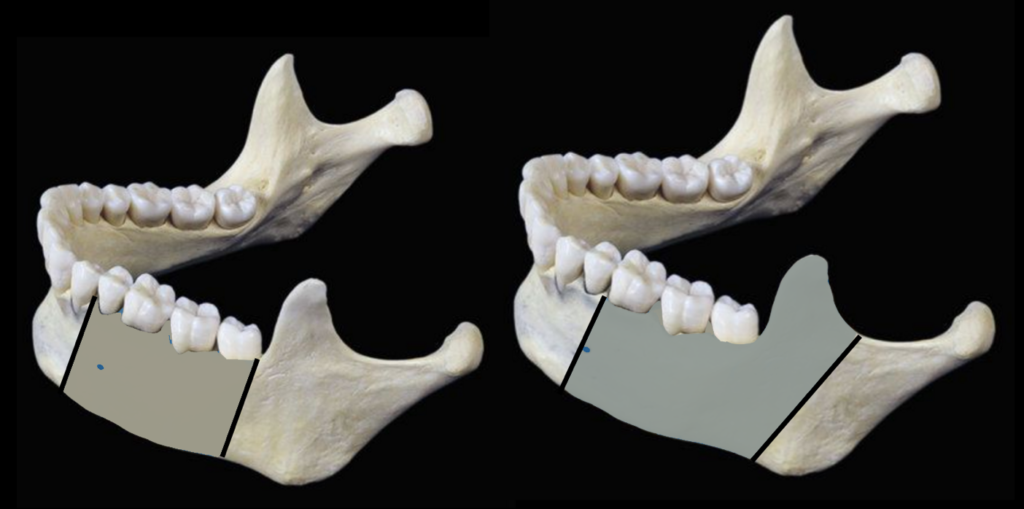
Fig.8. Segmental mandibulectomy. Shaded area of bone is removed. Needs reconstruc-tion of bone.
For large primary tumour, after resection of the tumour (Fig.8), at Apollo Cancer Centre, the resected areas are reconstructed using microvascular technique.
The lower jaw bone (mandible), which gives shape to the lower part of the face, is essen-tial for chewing food. This bone is removed when the tumour invades it. If the bone is not reconstructed, chewing food is difficult and the facial appearance also changes. Current-ly, the lower jaw is reconstructed with a bone from the leg (fibula) using microvascular technique. It helps in retaining the facial contour and the patient is able to chew well with the remaining teeth. Teeth can also be fixed onto titanium screws that are implanted into the bone either at the time of the primary surgery or later ( known as Osseo-integrated dental implants). VIDEO 01 Removal of fibula bone from the leg does not change the ap-pearance or function of the leg.
Recent Advances in lower jaw reconstruction
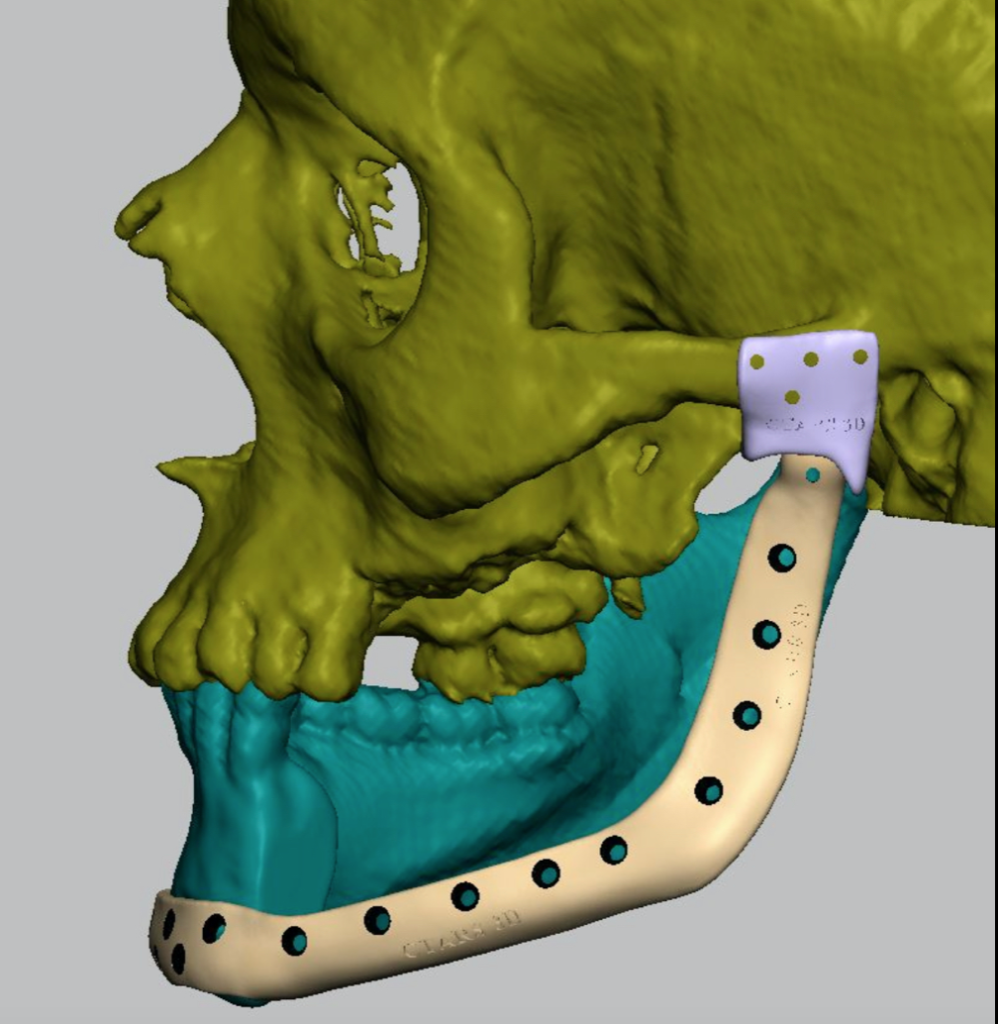
The lower jaw articulates with the skull. Its a ball and socket joint similar to hip joint. Based on the patient’s CT scan images, the reconstruction plate for the mandible (lower jaw) with condyle is custom made with medical grade titanium and the fossa (socket) is made using ultra molecular weight polyethylene using 3D printer (Fig.9).
Fig.9. 3D planning for mandibular reconstruction plate and articular fossa
Reconstruction of tongue
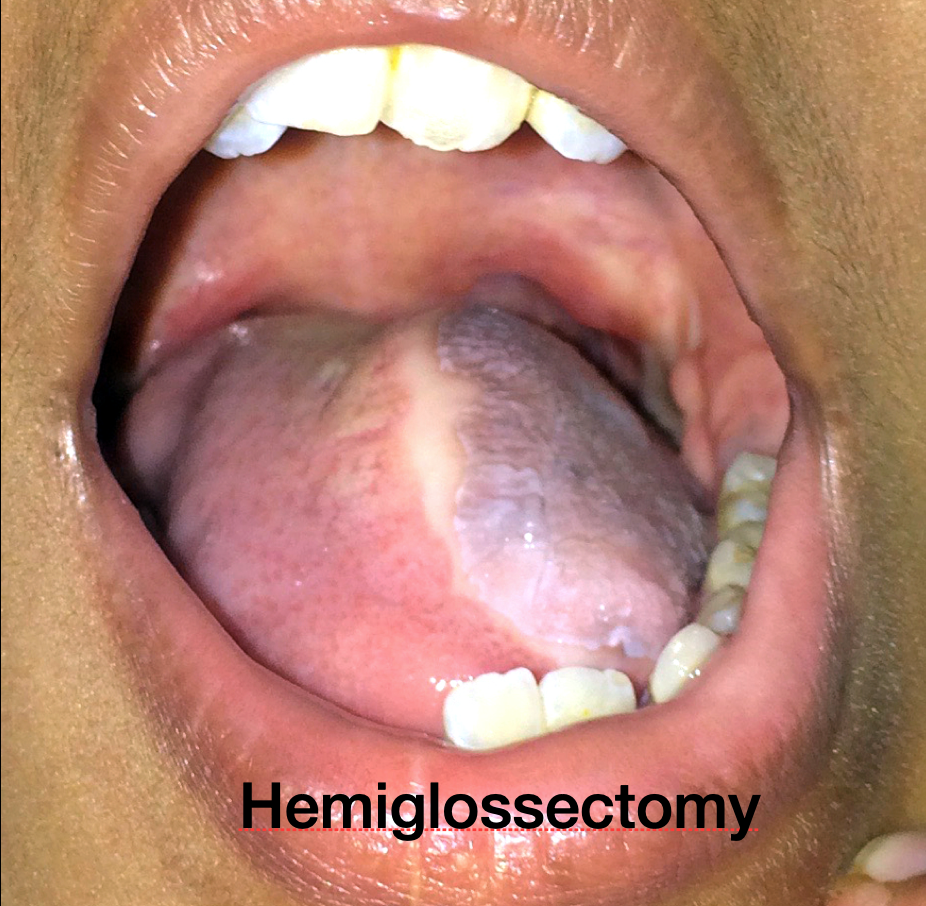
Fig.10a – Hemiglossectomy

Fig.10b – Subtotal glossectomy
the defect is immediately reconstructed using microvascular technique (Fig.10a & b) to improve speech and swallowing VIDEO 02.
Infratemporal fossa clearance
Some of these tumours can extend to involve the muscles used for chewing/mastication (pterygoid muscles) in infra temporal fossa. It was considered inoperable and therefore incurable. They were receiving palliative treatment. In the last 2 decades, considerable progress is made in resecting these tumours. This has improved the survival in these pa-tients.
Dr. Rayappa at Apollo Cancer Centre, Chennai is one of the pioneers in this field in this country and he is able to increase the survival of his patients from 0% to 40%
Follow-up Care:
Regular follow-up examinations are very important for anyone who has been treated for oral cancer. The doctor will watch the patient closely to check the healing process and to look for signs that the cancer may have returned. Patients with dryness of mouth from ra-diotherapy should have regular dental examination. The patient may need to see a dieti-tian if weight loss or eating problem continues. Oral cancer patients are strongly advised to stop using tobacco and limit alcohol intake to reduce the risk of developing another cancer.
Questions patients should ask before deciding about the treatment:
- What are my treatment options?
- What are the risks and benefits for each of my treatment options?
- How will treatment affect my everyday activity? How long?
- How often will I need to return?
- Has my doctor explained various surgical options to my satisfaction?
- Has a surgeon who has expertise with removal of cancer seen me?
- Have I seen by a radiation oncologist?
- Have I seen by a prosthodontist?
- Do I know all I need to know about speech rehabilitation techniques?
- How often has the surgeon performed the kind of surgery he is recommending?
- What will the surgical site look like after healing?
- Will my appearance and physical capabilities be affected? If so how?
- Should I consider combination therapy (both surgery and radiation therapy)?
The Heart Of Clinic

Dr. C. Rayappa MBBS, DLO, FRCS(Edin)
SENIOR CONSULTANT
+91 44 3315 1105
Dr. C. Rayappa graduated from Madras Medical College, Chennai, India in 1982. He completed his post graduation in Otolaryngology (ENT)
For Doctors
Need more information?
Reach us through mail or phone
The Heart Of Clinic
Dr. C. Rayappa MBBS, DLO, FRCS(Edin)
SENIOR CONSULTANT
+91 44 3315 1105
Dr. C. Rayappa graduated from Madras Medical College, Chennai, India in 1982. He completed his post graduation in Otolaryngology (ENT)