Cancer of Paranasal Sinus
Head and Neck Tumour Surgery
Sinus Cancer
Where are the sinuses?
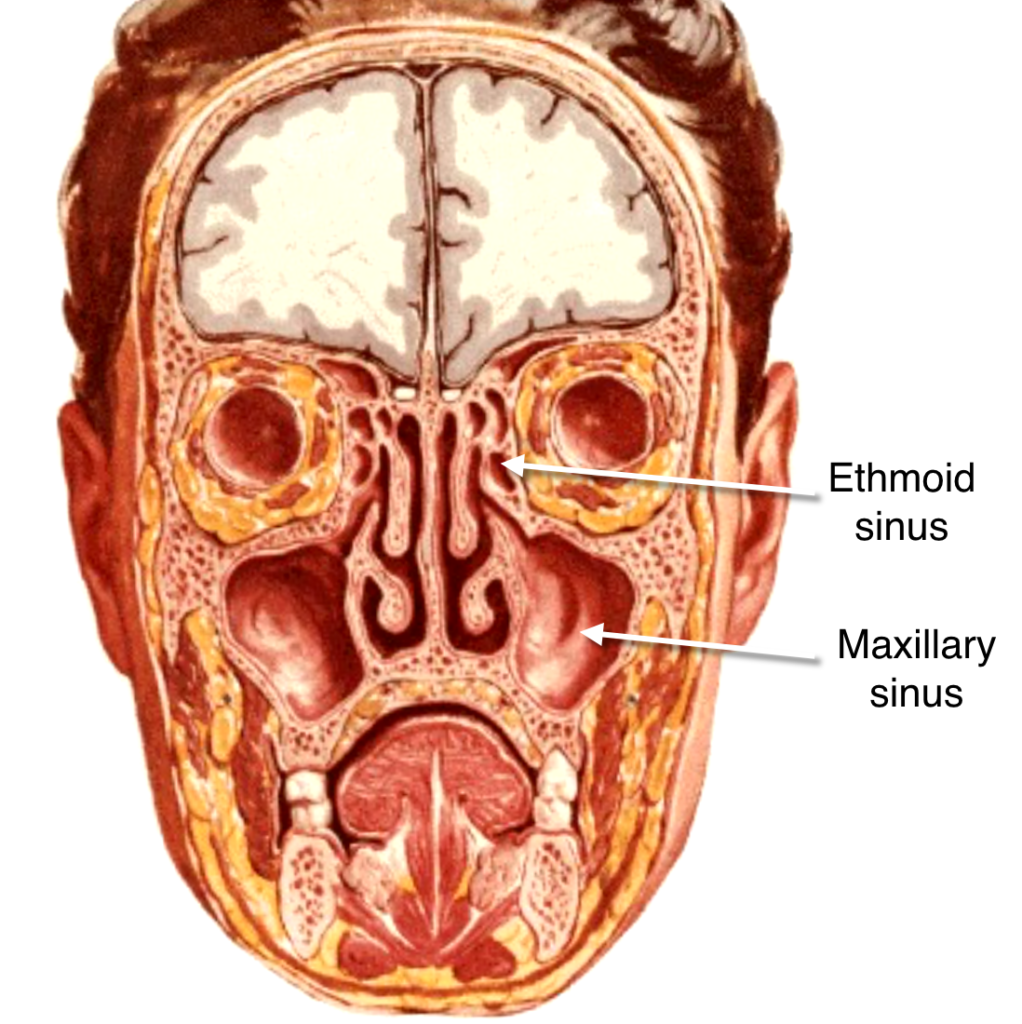
The paranasal sinuses are small hollow spaces in the bones
around the nose. There are several paranasal sinuses (Fig.1). A pair of frontal sinuses present above the nose, in the forehead. Largest of all, the maxillary sinus, present in the upper jaw one either side of nose and below the eyes. The ethmoid sinuses are present between the two eyes and the sphenoid sinuses lie behind the nose.
The sinuses and nose are lined with cells that produce mucous, which keeps the nose moist; the sinuses are also a space through which the voice can echo to make sounds when a person talks or sings. The nasal cavity is the passageway just behind the nostrils through which air passes on the way to the throat during breathing.
Types of sinus tumours and Whom does it affect?
Malignant tumours of the sinonasal tract are very uncommon, occurring in approximately 1 in 100,000 people and representing only 3% of all head and neck cancers. The incidence in males is twice that of females, due to the fact of a greater occupational exposure to certain carcinogens. These tumours most frequently develop during the 5th to 7th decades. About 80% of paranasal sinus cancers originate in the maxillary sinus. However, because a majority of them present at advanced stages, it is sometimes difficult to determine the exact primary site of the tumour.
Risk Factors:
- Tobacco smoking
- Occupational exposure of carcinogens
There is a significant high incidence of adenocarcinoma of the paranasal sinus among the furniture workers with chronic exposure to wood dust and in leather tanning industry. Nickel and chromium refining process have been implicated in the development of squamous cell and anaplastic cancer. Snuff and thorium dioxide, a radiological contrast agent, also have been associated with an increased incidence of sinonasal cancer.
What symptoms does it cause?
- Nasal obstruction that does not clear
- Nasal bleeding
- Headache or pain in the sinus region
- Pain in the upper teeth
- Problems with dentures
- Swelling or trouble with the eyes
- A lump or sore that does not heal inside the nose
- Swelling in the cheek
Because these symptoms are similar to those of chronic sinusitis, there is always a big delay between the onset of symptoms and final diagnosis. As a result, most patients usually present at late stages.
How is it diagnosed?
Anyone with such symptoms requires careful evaluation and examination with fibreoptic endoscopy. If an abnormal tissue is found, the doctor need to cut out a small piece and look at it under the microscope to see if there are any cancer cells. This is called a biopsy. Sometimes the doctor will need to cut into sinus to do a biopsy. CT scan helps to find out the extent of the mass, bone destruction and to find out whether it is involving the eye or extending intracranially (inside the skull). MRI scan gives better picture of intracranial extension, orbital involvement, perineural spread (adenoid cystic carcinoma spreads along the nerve) and differentiates an obstructed sinus with fluid collection from a space-occupying lesion.
How is it treated?
Currently most of the early carcinomas of the sinus are treated by surgery alone, whereas large lesions are treated by a combination of surgery and radiotherapy.
Surgery
- A number of surgical procedures available viz.
- Medial Maxillectomy
- Infrastructure Maxillectomy
- Total Maxillectomy
- Total Maxillectomy with orbital exenteration
- Total maxillectomy with infratemporal fossa clearance
- Craniofacial resection
- Endoscopic Craniofacial resection
In medial maxillectomy, only the lateral wall of the nasal cavity is removed. In infrastructure maxillectomy, only the lower part of the maxillary antrum, bearing the teeth was removed. Whereas in total maxillectomy whole of maxilla (upper jaw) is removed. This leaves a defect in the hard palate, which makes it difficult to talk and eat. This problem can be overcome by wearing a prosthesis made by the dentist. Since teeth can be fit into this prosthesis, it gives a good functional and cosmetic result. This prosthesis needs removal and cleaning by the patient. The current and preferable technique is to close the defect in the palate permanently using micro vascular flaps by the plastic surgeon. Osseo-integrated dental implants can be inserted later.
Tumours reaching the skull base or extending into the infratemporal fossa were considered inoperable and therefore incurable. With the current techniques of skull base surgery, these tumours are removed safely and completely (Craniofacial resection). This requires a team approach wherein ENT-Head & Neck Surgeon, Neurosurgeon and Plastic surgeon join together to remove these skull base tumours safely and reconstruct in such a way to bring function as well as appearance as close to normal as possible.
Infratemporal fossa clearance
Some of these tumours can extend to involve the muscles used for chewing/mastication (pterygoid muscles) in infra temporal fossa. It was considered inoperable and therefore incurable. They were receiving palliative treatment. In the last 2 decades, considerable progress is made in resecting these tumours. This has improved the survival in these patients.
Dr. Rayappa at Apollo Cancer Centre, Chennai is one of the pioneers in this field in this country and he is able to increase the survival of his patients from 0% to 40%
Recent Advances
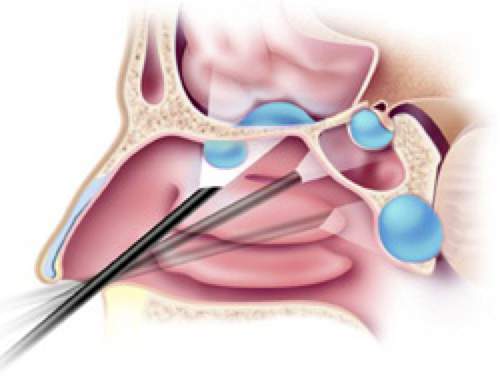
With newer endoscopic skull base surgical techniques, surgeons can completely remove ethmoid malignant tumours, without opening the skull (craniotomy) and retracting the unaffected normal brain. Covering of the brain (dura) is also excised and repaired endoscopically VIDEO. Endoscopic craniofacial resection has the advantages of completely removing the tumour without facial scar or opening the skull (craniotomy). The complications associated with brain retraction in open surgery are avoided. This is appropriate only for a small tumours.
Questions patients should ask before deciding about the treatment:
- What are my treatment options?
- What are the risks and benefits for each of my treatment options?
- How will treatment affect my everyday activity? How long?
- How often will I need to return?
- Has my doctor explained various surgical options to my satisfaction?
- Has a surgeon who has expertise with removal of cancer seen me?
- Have I seen by a radiation oncologist?
- Have I seen by a prosthodontist?
- Do I know all I need to know about speech rehabilitation techniques?
- How often has the surgeon performed the kind of surgery he is recommending?
- What will the surgical site look like after healing?
- Will my appearance and physical capabilities be affected? If so how?
- Should I consider combination therapy (both surgery and radiation therapy)?
The Heart Of Clinic

Dr. C. Rayappa MBBS, DLO, FRCS(Edin)
SENIOR CONSULTANT
+91 44 3315 1105
Dr. C. Rayappa graduated from Madras Medical College, Chennai, India in 1982. He completed his post graduation in Otolaryngology (ENT)
For Doctors
Need more information?
Reach us through mail or phone
The Heart Of Clinic
Dr. C. Rayappa MBBS, DLO, FRCS(Edin)
SENIOR CONSULTANT
+91 44 3315 1105
Dr. C. Rayappa graduated from Madras Medical College, Chennai, India in 1982. He completed his post graduation in Otolaryngology (ENT)