Temporal Bone Resection
Temporal Bone Resection
The treatment for temporal bone cancers is surgery and radiotherapy. Depending on the stage of the cancer, patient may also have chemotherapy.
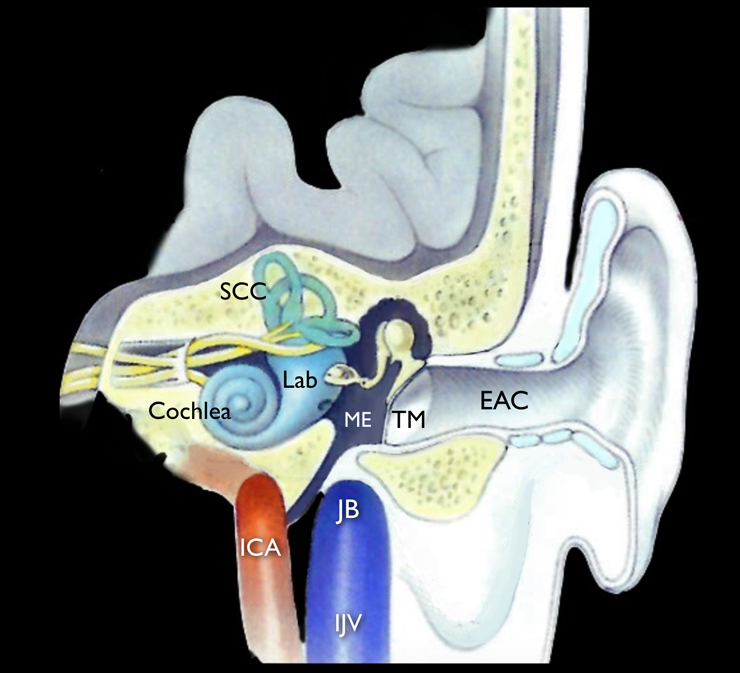
The type and extent of surgery needed depends on the area of ear (Fig.1) affected, and whether it has spread into nearby structures, such as the bone, dura, parotid etc. Surgeon will remove the tumour together with an area of tissue surrounding it that is completely free of cancer cells. Doing this helps to lower the risk of the cancer coming back.
- Surgery may involve having some or all of the following removed
- The Ear Canal
- Part or all of the temporal bone
- The Middle Ear
- The Inner Ear
The operations to remove the temporal bone tumour may range from a mastoidectomy to total temporal bone resection. They may also need to remove the lymph nodes nearby in the neck and the salivary gland on that side of the head. Rarely, surgeon may need to remove the facial nerve, which runs through the temporal bone. In that case, nerve grafting is done to regain the facial movement.
If the middle and inner ear were removed it is unlikely that the patient will be able to hear on that side. Balance may be affected and the patient may feel dizzy temporarily. Sometimes it is possible for the surgeon to rebuild (reconstruct) some of the ear so that hearing can be preserved. With this operation, appearance won’t change for most people. Scar line is likely to be behind the ear.
Intraoperative Details
Management of the primary site

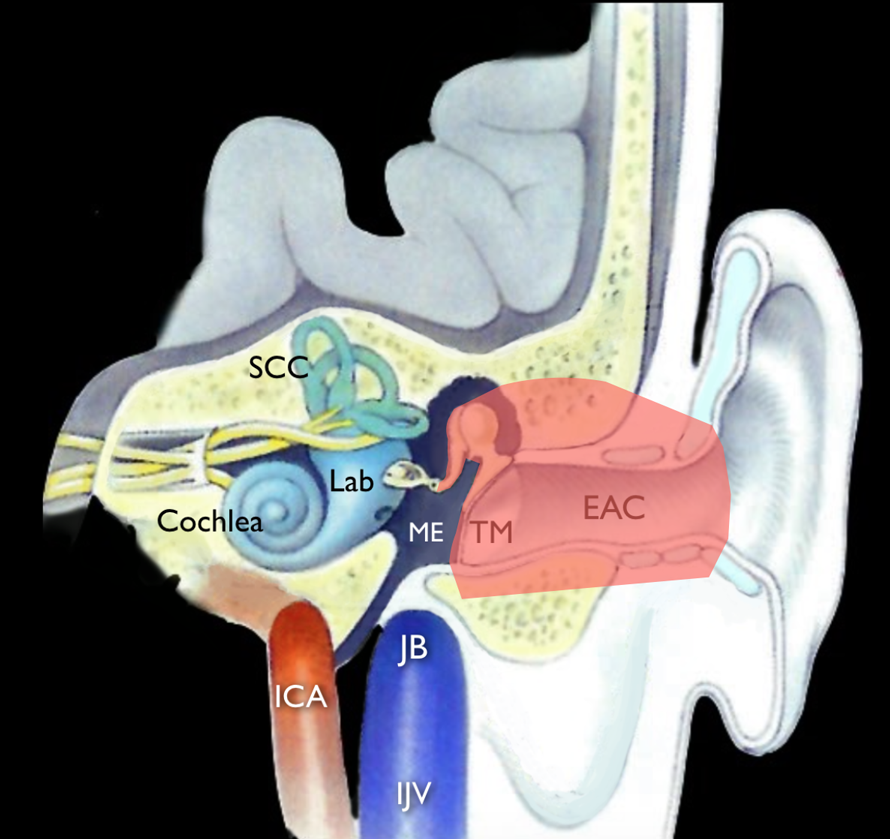
For tumours limited to external auditory canal, Lateral Temporal Bone Resection (LTBR) is done. The LTBR includes resection of the EAC, tympanic membrane, malleus, and incus (Fig.2). The boundaries are the middle ear cavity and stapes medially, the mastoid cavity posteriorly, the epitympanum and zygomatic root superiorly, the Temporomandibular Joint (TMJ) capsule anteriorly, and the medial tympanic ring or Infratemporal Fossa (ITF) inferiorly. The lateral margin depends on the extent of spread. The otic capsule and facial nerve are preserved. The LTBR is appropriate for T1 and T2 tumours.
The LTBR begins with a long, postauricular incision extending from the temporal fossa into the neck. If the pinna is to be preserved, a second incision is made within the concha lateral to the lesion. If the pinna is to be resected, a preauricular incision is incorporated to the postauricular incision allowing the pinna and surrounding skin to be included in the specimen. A cortical mastoidectomy is performed and the facial nerve identified. Bone removal is extended into the zygomatic root and to the digastric ridge. An extended facial recess is made, and the incudostapedial joint is separated. The facial recess is continued inferiorly and anteriorly lateral to the facial nerve, but medial to the annulus, until the specimen is attached only at the anterior canal bony wall at the level of the temporomandibular capsule. An osteotome is used to separate the bony specimen. The parotidectomy is performed en bloc.
Medina (1990) described several modifications of the lateral temporal bone dissection based on the location of disease. A modified LTBR removes the EAC and leaves the uninvolved tympanic membrane intact. This type of resection is appropriate for tumours originating in the concha without involvement of the EAC.
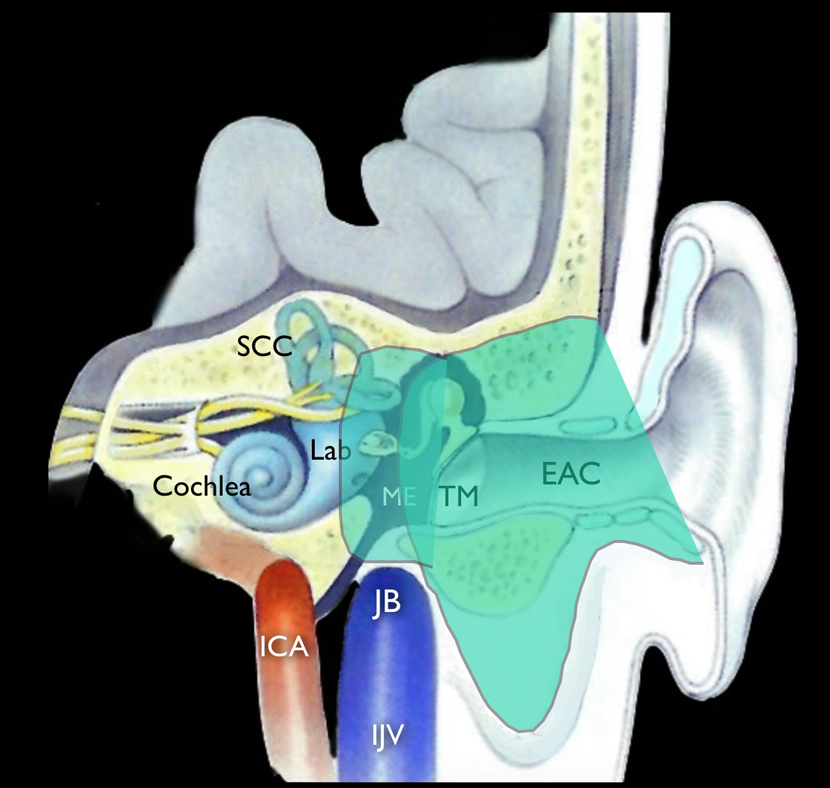
A Subtotal Temporal Bone Resection (STBR) is performed when invasion medial to the tympanic membrane or into the mastoid (T3 disease) is evident. In this case, the medial margin may be obtained in a piecemeal fashion, usually with a drill. The specimen includes the LTBR with additional dissection of the otic capsule and the medial bony wall of the middle ear and mastoid (Fig.3). The margins of resection are the sigmoid sinus and posterior fossa dura posteriorly, middle fossa dura superiorly, internal carotid artery anteriorly, jugular bulb inferiorly, and petrous apex medially.
Based on the extent of tumour spread, dissection may include the condyle of the mandible, the facial nerve, dura, sigmoid sinus, and contents of the infratemporal fossa. The carotid artery is skeletonized and becomes the medial margin.
Tumour involvement of the jugular bulb requires ligation of the inferior jugular vein and proximal control of the sigmoid sinus. The facial nerve is traditionally sacrificed, with the proximal margin taken in the labyrinthine or internal auditory canal segment. However, the surgeon may elect to preserve the nerve if no indication of nerve involvement exists. The medial extent of dissection at the level of the otic capsule depends on the depth of involvement and is done piecemeal. Tumour extension into the protympanum, eustachian tube, or carotid artery is addressed with an infratemporal fossa dissection. The temporalis muscle is reflected and the zygomatic arch removed. The mandibular condyle is resected. The dissection proceeds based on the extent of disease but may include identification of the pterygoid plate, the mandibular nerve (V3), and the horizontal carotid artery and may include a temporal craniotomy.
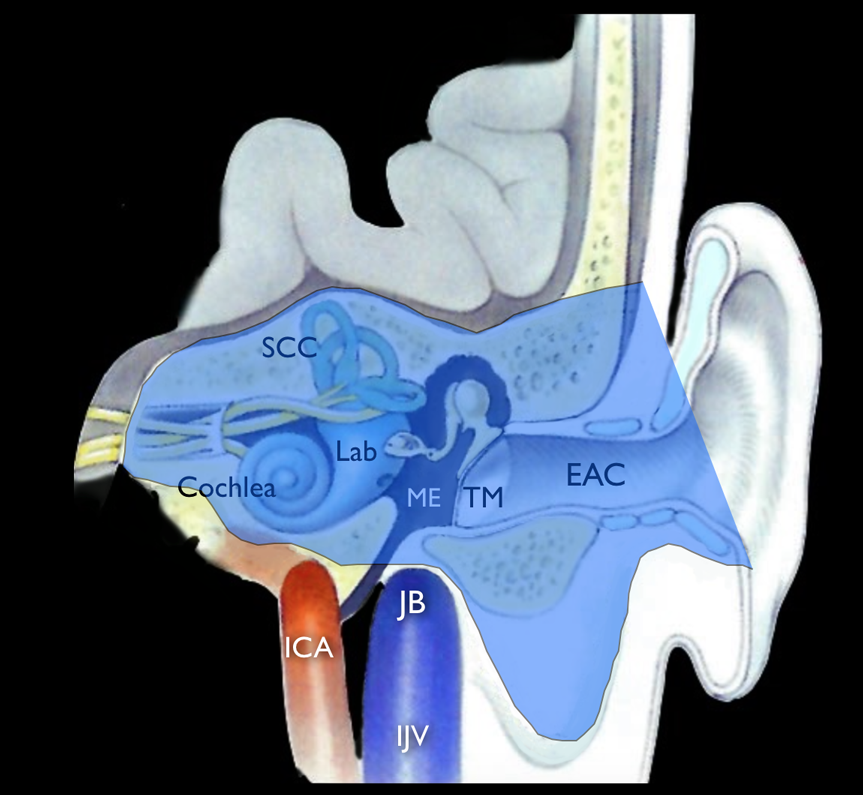
A Total Temporal Bone Resection (Fig.4) can be used to address T4 disease. However, this procedure is associated with significant morbidity and may not significantly improve survival in these cases of advanced disease. The resection includes the STBR with the additional resection of the petrous apex. The internal carotid artery may be isolated, mobilized, and preserved or resected. The sigmoid sinus, jugular vein, carotid artery, dura and CNs are removed as indicated by the extent of the tumour.
Management of the parotid and temporomandibular joint
The intraparotid lymph nodes are a first echelon drainage site for cancers of the EAC and middle ear. An adequate anterior margin for the temporal bone resection routinely involves resection of the parotid gland, temporomandibular joint, and condyle. Resection of these soft tissues will also address minimal soft tissue extension beyond the temporal bone. Ideally, this is performed en bloc with the temporal bone. A superficial parotidectomy is performed with preservation of the facial nerve for T1 and T2 tumours. When the facial nerve is resected for more advanced lesions, a total parotidectomy may be performed.
Management of the dura and brain
Although involvement of the dura and brain carry a poor prognosis, an aggressive approach includes resection of the dura and a small volume of the temporal lobe with a healthy margin.
Reconstruction
Management of facial nerve paralysis may include CN XII to VII grafting, cross facial grafting, and static procedures. Extensive resections may result in large soft tissue defects. A temporalis muscle flap can be used to fill small to medium defects. The pedicled myocutaneous trapezius flap is an excellent option for reconstruction of the soft tissue and skin defect. The pectoralis flap has limited distant reach to the resected margin. The anterolateral thigh free flap and rectus abdominis free flap are particularly suited for the area. Dural defects should be repaired primarily or with graft reconstruction.
The Heart Of Clinic

Dr. C. Rayappa MBBS, DLO, FRCS(Edin)
SENIOR CONSULTANT
+91 44 3315 1105
Dr. C. Rayappa graduated from Madras Medical College, Chennai, India in 1982. He completed his post graduation in Otolaryngology (ENT)
For Doctors
Need more information?
Reach us through mail or phone
The Heart Of Clinic
Dr. C. Rayappa MBBS, DLO, FRCS(Edin)
SENIOR CONSULTANT
+91 44 3315 1105
Dr. C. Rayappa graduated from Madras Medical College, Chennai, India in 1982. He completed his post graduation in Otolaryngology (ENT)