CSF Rhinorrhoea & Meningocoele
Endoscopic SkullBase Surgery
CSF Rhinorrhoea & Meningocoele
Cerebrospinal fluid (CSF) is a clear, colourless liquid that fills and surrounds the brain and the spinal cord and is contained by the covering of brain (dura). When there is a hole in the dura and skullbase bone, CSF can then leak into the nose and sinuses. Sometimes, the dura herniates through the defect and is known as ‘meningocele’. If the defect is large, brain may also herniate through the defect and is known as ‘encephalocoele’.
CSF rhinorrhea is rare but can lead to meningitis, which may result in significant morbidity and mortality for the patient.
Causes of CSF leak
CSF leaks can happen following head injury, surgery (neurosurgery or sinus surgery) or may occur spontaneously. Traumatic causes include both blunt and penetrating facial injuries. Most spontaneous CSF rhinorrhea are now thought actually to be secondary to elevations in intracranial pressure (ICP). Congenital skull base defects and certain tumors can also lead to CSF rhinorrhea.
Clinical picture
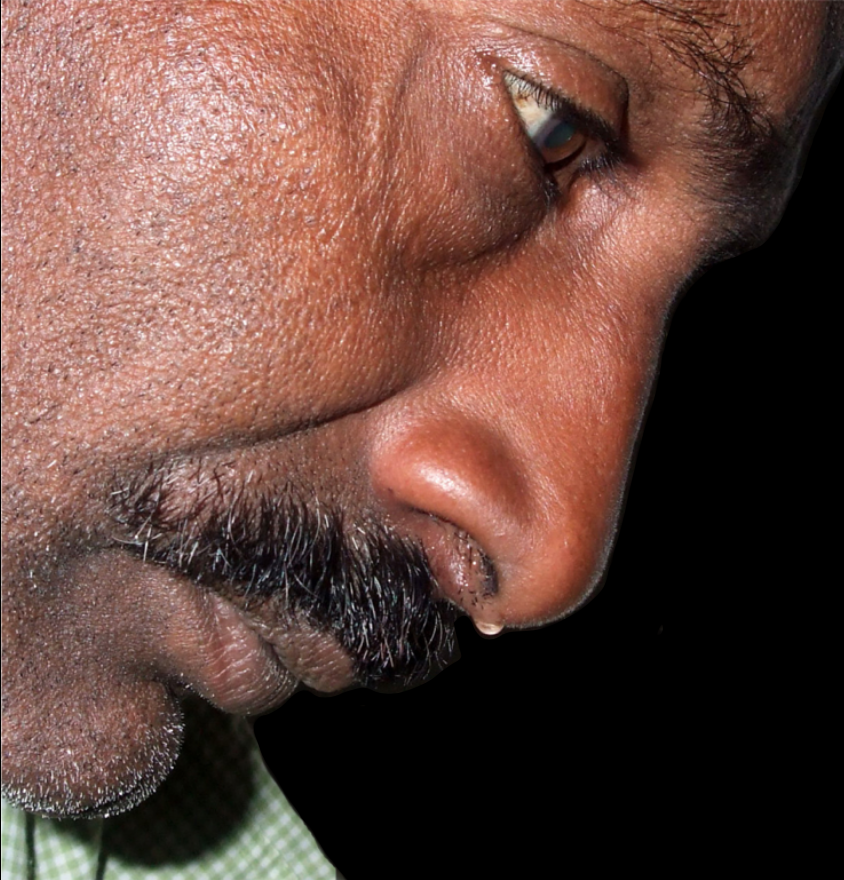
The typical history of a cerebropsinal fluid (CSF) leak is that of clear, watery discharge, usually unilateral (Fig.1). However if fluid drains into the back of the throat there may be a salty taste. Drainage also tends to increase when bending over or straining. If there is meningo-encephalocoele, in addition to CSF leak, it will cause obstructive symptoms in nose.
How is it diagnosed?
Diagnosis is made more easily in patients with recent trauma or surgery than in others. Patients with recurrent meningitis should be evaluated for a skull base defect regardless of the presence or absence of CSF rhinorrhea. Patients with herniation of dura and/or brain can have nasal obstruction.
Chemical analysis of the nasal fluid for glucose and protein but is unreliable. Beta2-transferrin is located only within the CSF, perilymph, and aqueous humor. This is currently single best laboratory test for identifying the presence of CSF in sinonasal fluid.
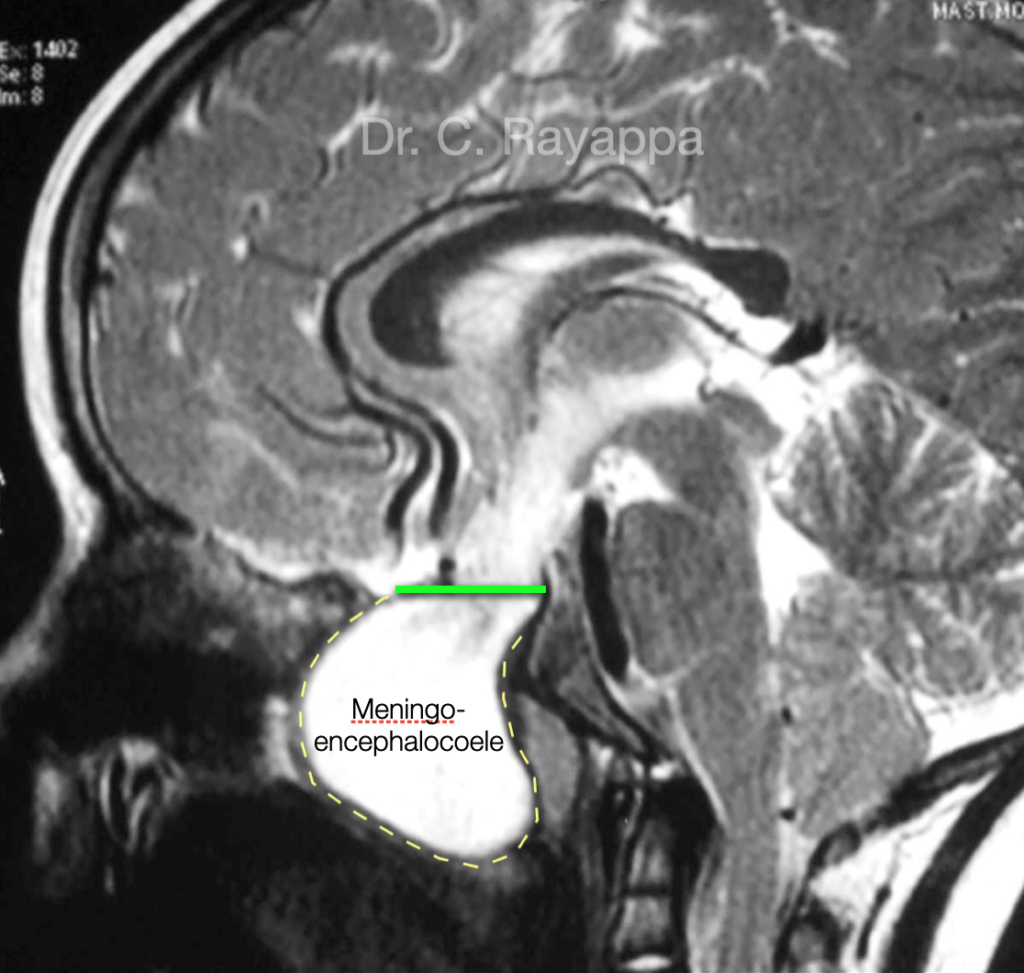
High-resolution CT scanning is the imaging modality of choice for identifying a skull base defect associated with CSF rhinorrhea. Injection of intrathecal contrast improves localization of the site of the CSF leak in most patients with active leak. Patients with intermittent CSF rhinorrhea may have false-negative CT cisternograms. Another disadvantage of this technique is that it may miss cribriform or ethmoid sinus defects. MRI shows the site of leak, encephalocele or meningocoele (Fig.2) and if there are signs of increased intracranial pressure.
Treatment of CSF Rhinorrhoea
As traumatic leaks stop spontaneously in the majority of cases, conservative measures (bed rest, stool softeners, and lumbar drainage) are taken for a period of 7 days. However, if CSF rhinorrhea persists beyond this point, or if a large skull base defect is observed at the time of injury, surgical repair is warranted.
Surgical repair is recommended in all patients with spontaneous or iatrogenic CSF rhinorrhea in order to prevent ascending meningitis. If an iatrogenic leak is detected intraoperatively, it should be repaired at the time of the original surgery. As only one third of spontaneous leaks stop spontaneously and intermittent leakage over several years is characteristic, surgery is the only option.
Traditionally, a large skull opening was required to see the site of the leak after lifting up the frontal lobe of the brain. Disadvantages of the intracranial approach include increased morbidity, loss of smell, and trauma related to brain retraction, including seizures, edema, and hemorrhage.

Now, with minimally invasive endoscopic techniques, the site of the fluid leak can be approached through the nose and fixed without opening up the skull or touching the brain. Endoscopic repair has now become the preferred method of controlling CSF rhinorrhea, with the high success rate of 90-95%. It avoids the morbidity associated with the open craniotomy approach. It has several advantages, including enhanced illumination and magnified as well as angled visualization. Another advantage is the ability to more accurately position the grafts (Fig.3). If the CSF pressure is high, to prevent recurrence, lumbo-peritoneal shunt is done.
Treatment of Nasal Meningo-encephalocoele
In cases of Encephalocoele treatment includes removing the herniated sac and repairing the skull opening. Encephalocoele of the skull base can be removed using the endoscope through the nose and nasal cavities (Fig.4 & 5). In transnasal endoscopic surgery, there are no incisions in the face or scalp, a shorter hospital stay and faster recovery.
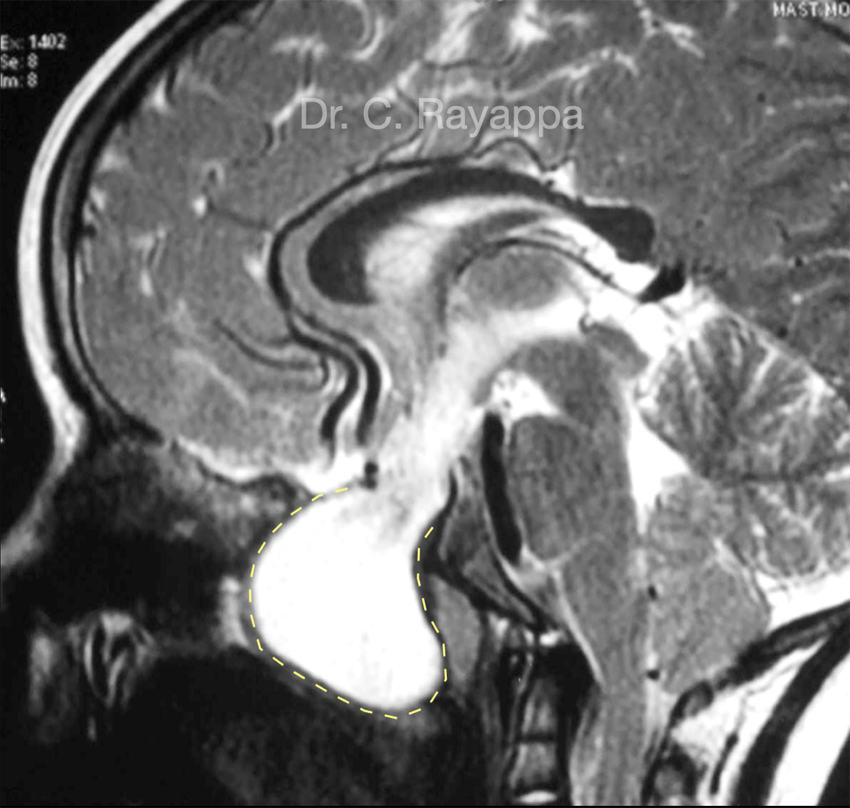
Fig.4. MRI shows a large meningoencephalocoele filling the nasal cavity and nasopharynx
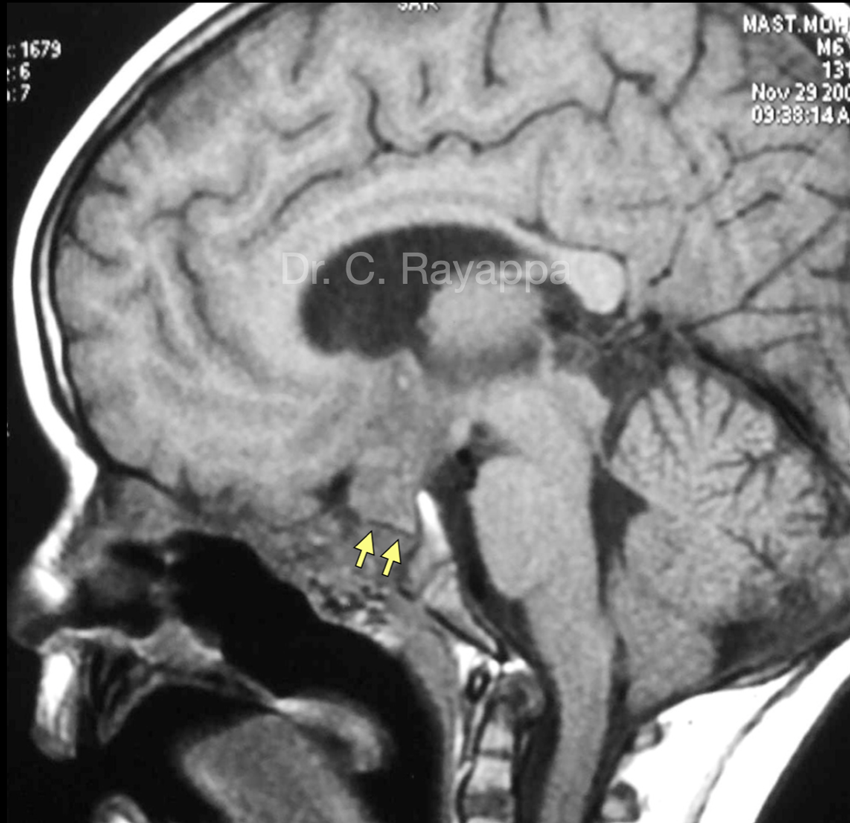
Fig.5. 1 yr post endoscopic repair. MRI shows good nasal airway, soft tissue covering the area of skull base repair. Yellow arrows pointing at a black line formed by the bone used to repair the skull base defect.
The Heart Of Clinic

Dr. C. Rayappa MBBS, DLO, FRCS(Edin)
SENIOR CONSULTANT
+91 44 3315 1105
Dr. C. Rayappa graduated from Madras Medical College, Chennai, India in 1982. He completed his post graduation in Otolaryngology (ENT)
For Doctors
Need more information?
Reach us through mail or phone
The Heart Of Clinic
Dr. C. Rayappa MBBS, DLO, FRCS(Edin)
SENIOR CONSULTANT
+91 44 3315 1105
Dr. C. Rayappa graduated from Madras Medical College, Chennai, India in 1982. He completed his post graduation in Otolaryngology (ENT)