Glomous Tumours (Paraganglioma)
Glomous Tumours (Paraganglioma)
Indications:
- Glomus tympanicum
- Glomus jugulare
- Glomus vagale
- Carotid body tumour
These are rare, slow-growing, very vascular tumours of a group called paragangliomas. They are derived from glomus bodies which themselves are derived from neural tissue. They occur at carotid bifurcation, the vagus nerve, top of internal jugular vein known as jugular bulb and the middle ear. Rarely, they may be found at other sites, including the periaortic area, trachea, larynx, mandible, nose, ciliary ganglion and Fallopian canal.
These tumours tend to be benign and slow growing but they can be locally aggressive. Malignancy is rare and only about 4% metastasise to the lung, lymph nodes, liver, vertebrae, ribs and spleen. Upto 3% of tumours produce adrenaline-like hormones, resulting in a clinical picture similar to phaeochromocytoma with hypertension and tachycardia.
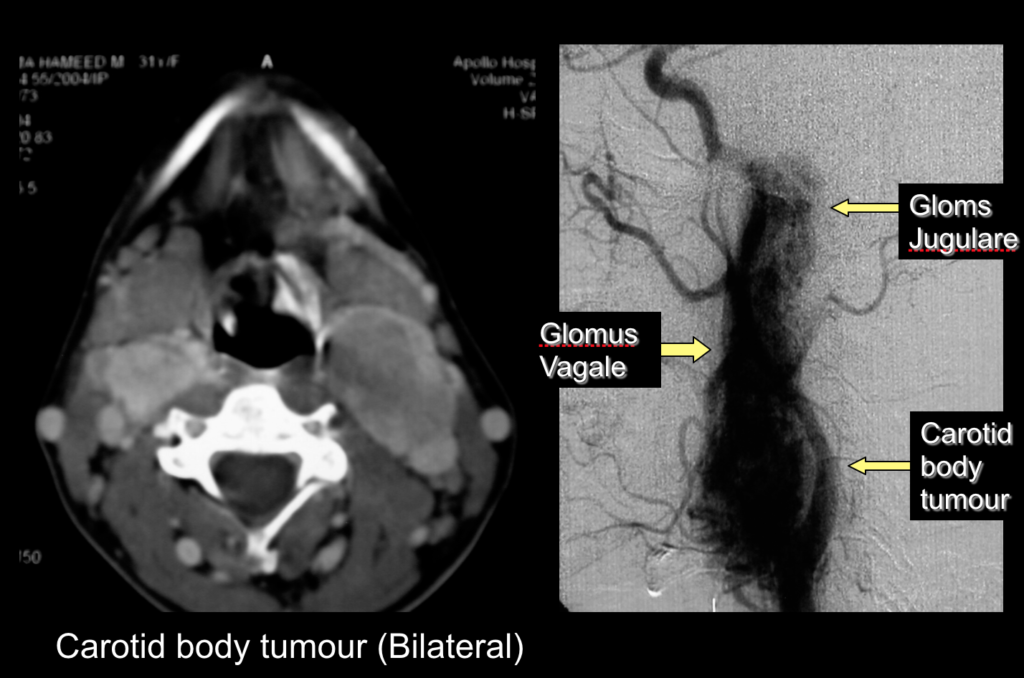
Fig. 1
This patient had carotid body tumour, glomus vagale and glomus jugulare on one side (CT and angiogram) and a small carotid body tumour on contralateral side (CT).
They sometimes run in families in an autosomal dominant fashion with incomplete penetrance. These tumours can arise at multiple sites(Fig.1). The incidence of multicentric origin is about 10% and it goes up to 50% in familial cases.
Glomusjugulare arises at the skull base in an area known as jugular foramen. A number of structures pass through this foramen viz. internal jugular vein that takes the impure blood from brain to the heart and three cranial nerves, which control the speech and swallowing. It is also closely related to the middle and inner ear. Therefore, the symptoms are related to loss of function of the ear and cranial nerves. These can include partial or complete hearing loss, a ringing or pulsing sound, which is called tinnitus and dizziness. If the tumour is large enough and grows towards the neck, it can causefacial paralysis, difficulty in swallowing, hoarseness, drooping shoulders and tongue weakness. In a small percentage of glomusjugularetumours, the mass may produce hormones and cause additional symptoms like headache, tremors, flushing, anxiety, high blood pressure and a rapid heart rate.
Investigations
- CT & MRI are done to know
- the site & extent of tumour, involvement of neurovascular structures
- presence of any other glomustumour
- Blood and urine tests are done to detect hormones that are produced in up to 3% of tumors. It is important to detect these hormones before surgical removal because the hormones can spill from the tumour during surgical removal and cause the blood pressure to rise to dangerous levels. If you are diagnosed to have a tumor, which produces these hormones, you will be given medications to protect you from the effects of spilled hormones during surgery.
Management
If the tumour is very small and limited to the space behind the eardrum (middle ear), the tumour is known as a glomustympanicum. These tumours are easily removed by lifting the eardrum through the ear canal. Surgery for glomustympanicumtumours can generally be done safely as an outpatient.
The management of glomusjugularetumours depends on a number of factors including age, overall health status, presenting symptoms, tumour size, and patient preference. Treatment options include observation, partial or total surgical removal, external beam radiation, or a combination of surgery and radiation therapy.
Observation with serial imaging studies (CT or MRI) is often recommended in patients with advanced age, multiple health issues, or according to patient preference.
The treatment of choice for a glomusjugularetumour is surgery. It may be completely removed using traditional skull base surgical techniques. The process is difficult because there are so many nerves in the area. These nerves control the muscles of the tongue, the throat, the vocal cords, and the shoulder, and are at risk for injury during surgery. State of the art intraoperative nerve monitoring techniques are utilized to minimize nerve trauma during tumour removal. If the tumour can be taken out without damaging any nerves, no other treatment is needed. Complete surgical removal is typically recommended in younger patients. Temporary facial weakness is the most common side effect in the removal of these tumours because the facial nerve often has to be moved out of its normal position to allow direct access to the jugular foramen.
These tumours are highly vascular and excessive blood loss happens during surgery. In recent years, the neuroradiologist does carotid angiography 24 to 48 hours before surgery, finds the blood vessel that feeds the tumour and blocks it. It is known as embolization. This reduces the bleeding during surgery and the procedure can be performed with greater safety. Also the preservation of vital structures around the tumour is enhanced, including cranial nerves going to the throat, vocal cords and face.
If the tumour is adherent to internal carotid artery or to the cranial nerves that are functioning (normal swallowing function, shoulder function, tongue movement and voice), a small amount of tumour may be left on these structures to reduce morbidity and this residual tumour can be taken care with postoperative radiotherapy. Radiation treatment can be used as primary therapyfor patients who are not fit for surgery or following recurrence or planned partial excision.
Glomusvagale
Glomus tumour which occur in the upper part of neck typically arise along a nerve called the vagus nerve, which controls the movement of vocal cord and is known as glomusvagale. Usually present with change in the voice caused by injury to the vagus nerve. Surgery for a glomusvagaletumour is generally done through an incision high in the neck.
Carotid Body Tumor
If the tumour occurs at the level of the bifurcation of the carotid artery, it is called a carotid body tumour. These are typically noticed first as a soft lump in the neck. Surgery for a carotid body tumour is done through an incision in the neck, and rarely causes any nerve problems. The tumour is dissected off the internal, external and common carotid arteries. In large tumours, the tumour may be adherent to the internal carotid artery which may necessitate resection and grafting of internal carotid artery.
The Heart Of Clinic

Dr. C. Rayappa MBBS, DLO, FRCS(Edin)
SENIOR CONSULTANT
+91 44 3315 1105
Dr. C. Rayappa graduated from Madras Medical College, Chennai, India in 1982. He completed his post graduation in Otolaryngology (ENT)
For Doctors
Need more information?
Reach us through mail or phone
The Heart Of Clinic
Dr. C. Rayappa MBBS, DLO, FRCS(Edin)
SENIOR CONSULTANT
+91 44 3315 1105
Dr. C. Rayappa graduated from Madras Medical College, Chennai, India in 1982. He completed his post graduation in Otolaryngology (ENT)