Cancer of Larynx
Head and Neck Tumour Surgery
Cancer of Larynx
Where is Larynx (voice box)?
The larynx or voice box is located in the neck. The large cartilage that forms the front of the larynx produces a sharp bulge in the neck in men and is called the ‘Adams apple’. It contains the vocal cords and the muscles, which move them. The vocal cords vibrate and make sound when air is directed against them. The sound echoes through pharynx, mouth, nose and sinuses to make a person’s voice. Air passes through the pharynx, then the larynx on the way to the windpipe and lungs. The food passes through the pharynx to the oesophagus. The larynx has a leaf like structure called epiglottis, which prevents the food going into the airway. (Fig. 1 & 2)

Fig.1. Adam’s apple
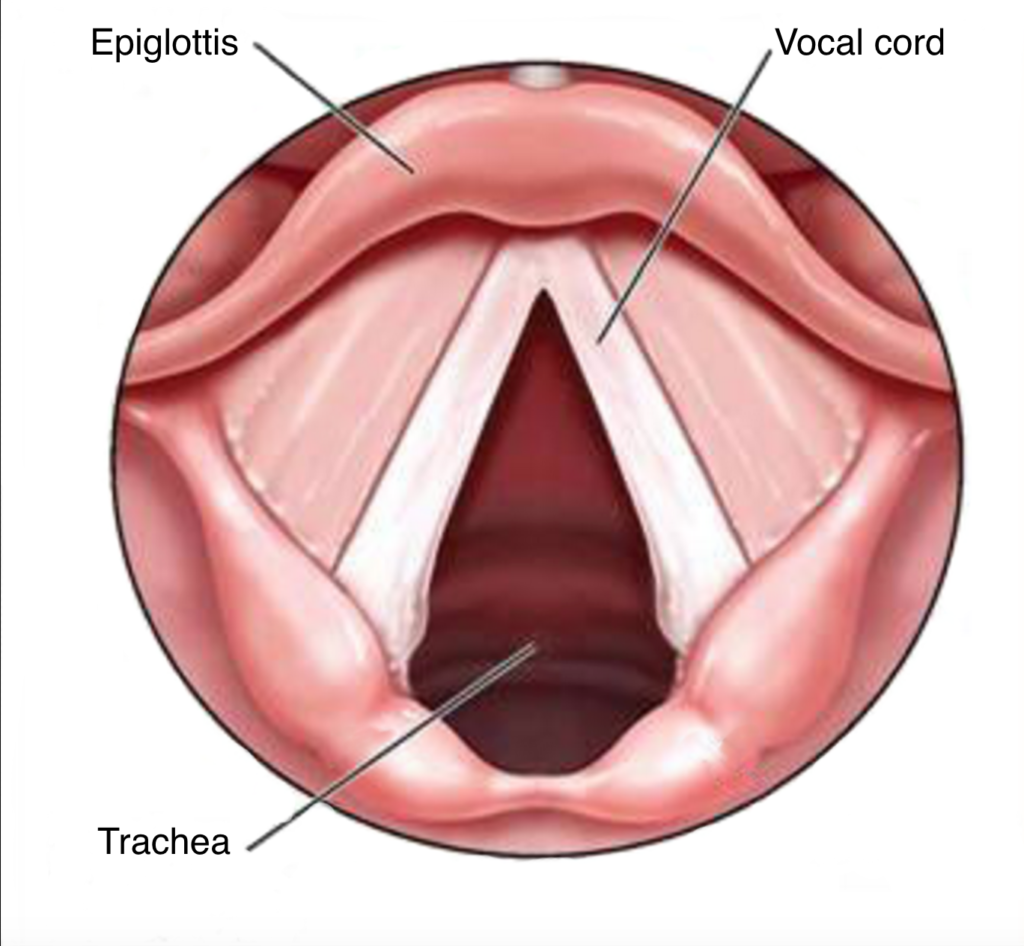
Fig.2. Larynx
The Larynx include the:
- Vocal cords (glottis)
- Area above the vocal cords, including epiglottis (supraglottis), and
- Area below the vocal cords (subglottis) that connects the larynx to the wind pipe (trachea)
Like other parts of the body, the larynx is made up of many types of cells. When cells divide in an abnormal, uncontrolled way, they can form a non-cancerous (benign) or cancerous (malignant) tumour. Approximately 95% of laryngeal cancers are squamous cell cancers arising from the mucous membranes. Cancers forming in the glands and connective tissues of the larynx are rare.
Who does it affect?
Cancers of the larynx is especially common in smokers. It is typical for the cancers of the squamous cells of the larynx to begin as pre-cancerous conditions, such as an abnormal growth (dysplaisa). Not all pre-cancerous conditions develop into cancer. They sometimes go away without treatment, especially if the person stops smoking or eliminates other risk factors. Approximately 25% of patients diagnosed with laryngeal cancers have another cancer in a nearby area, such as mouth, oesophagus or lung. Another 15% will later develop cancer in one of these areas. That’s why patients should continue with follow-up examinations throughout their lifetime.
Risk Factors
- Use of Tobacco Products
This includes cigarettes and smokeless tobacco. Smokers are 5 to 35 times more likely to develop laryngeal cancers than non-smokers. Statistics show that 37 % of head and neck cancer patients who continue smoking will develop a recurrent tumour or second cancer. Compare that to only 6% of the head and neck cancer recurrence in patients who stop smoking.
- Excessive Consumption of Alcohol
- Occupational Hazard
Over exposure to paint fumes, wood dust; some chemicals and even asbestos may increase the risk of developing laryngeal cancers.
What symptoms does it cause?
An ENT surgeon should be seen if any of the following symptoms exist for more than two weeks. Pain is not an early symptom. Symptoms of laryngeal cancer include:
- Hoarseness of voice
- A lump in the neck
- A sore throat or ear ache
- Difficulty in breathing
- Pain and difficulty in swallowing
Most of the cancers of the larynx begin on the vocal cords (atleast 70%). These tumours are seldom painful, but they almost always cause hoarseness. Tumours that begin in the area below the vocal cords are rare. Such tumours can make it hard to breathe. Breathing may even become noisy.
Early detection of laryngeal cancer is important because treatment is most effective before the disease has spread. These types of cancers usually spread to lymph nodes in the neck, the back of the tongue, other parts of the throat and neck and the lungs. Spread of cancer to lymph nodes of patients with true cord cancer is extremely rare. The reverse is true for patients with supraglottic cancers, where up to 40% of patients will have some spread of cancer to the lymph nodes of the neck.
How is it diagnosed?
The ENT surgeon with the help of small mirrors or a fibreoptic endoscope will examine the larynx. The fibreoptic flexible laryngoscopy can be done as an outpatient procedure under local anesthesia by passing a thin endoscope through the nose in to the pharynx.
If something suspicious is seen, then the next step is doing endoscopy under general anesthesia. The larynx is examined with the help an operating microscope (Microlaryngoscopy). If some area looks abnormal, then biopsy is done from that area.
If neck nodes are enlarged, fine needle aspiration is done for cytological examination (FNAC) by the pathologist to rule out metastatic carcinoma. If cancer is found, the doctor will need to know the extent of the disease. This is called staging. In most cases, the most important factor in considering treatment options is the stage of the disease. The stage is based on the size of the tumour, as well as whether or not the cancer has spread (metastasized) and where it has spread. To obtain more information about the location and extent of the cancer, the doctor may perform the following investigations.
- CT scan / MRI of neck
- PET - CT
How is it treated?
Treatment Options
Treatment of small cancers of the larynx usually results in a good outcome. The cure rate for such a cancer that has not spread is 75-95 percent.
Radiation often is the first treatment option for this type of cancer because this helps to preserve the voice. Advanced laryngeal cancer may be treated with chemotherapy and radiation therapy in an effort to avoid surgical removal of the larynx (Organ preservation protocol).
Surgery may also be needed later if the cancer recurs. There are numerous surgical procedures now available that result in just partial removal of the voice box in order to retain normal breathing patterns and speaking. The treatment plan should be individualized depending on the location of the cancer, its size, the stage of the disease and the patient’s general health.
Surgery
Surgery for cancer if the larynx involves removal of the affected portion of the larynx with significant normal healthy tissue around it. Complete surgical clearance of the tumour is achieved with the help of the pathologist who examines the removed tissue at the time of surgery (Frozen section) and says whether removal was complete or needs further removal.
- Patients with laryngeal cancer may undergo one of these types of surgeries.
- Cordectomy – removal of the vocal cord
- Supraglottis laryngectomy- removal of the supraglottis
- Partial laryngectomy – removal of part of the larynx
- Supracricoid laryngectomy with CHP or CHEP
- Transoral laser microsurgery
- Transoral robotic-assisted partial laryngectomy
- Total laryngectomy – removal of the entire larynx
VOICE PRESERVATION SURGERY
In voice preservation surgery, surgeon aims at preserving the uninvolved portion of larynx without compromising cancer clearance. Based on clinical examination as well as CT/MRI findings surgeon decides whether the patient is suitable for voice preservation surgery. With a partial laryngectomy, the surgeon creates a temporary breathing hole in the neck. The part of the larynx containing tumour is resected with sufficient normal tissue around it and then the larynx is reconstructed. Once the stoma closes, they are able to breathe normally and speak.
Transoral Laser Microsurgery (TLM) Assisted Partial Laryngectomy: (Fig.3)

Fig.3. Transoral laser microsurgery (TLM) assisted partial laryngectomy

This is a partial laryngectomy performed through the mouth. In this procedure, the voice box is exposed using special instruments. A laser attached to the microscope is used to cut out the tumour, with the aim of getting a margin of normal tissue around it. This remains an option for small primary or recurrent cancers after non-surgical therapy. (VIDEO 01)
Transoral Robotic-Assisted Partial Laryngectomy: (Fig.4) This procedure simply uses a robot to get exposure and to remove a tumour of the larynx through the mouth. The principles are the same as transoral laser microsurgery with the exception that the instruments are different.

Fig.4. Transoral Robotic-Assisted Partial Laryngectomy
Open Partial Laryngectomy: In small tumours, portion of the larynx involved by the tumour alone is resected without compromising cancer clearance. Various procedures viz. vertical partial laryngectomy (Video 02), supraglottic laryngectomy and supracricoid laryngectomy (cricohyoidopexy & cricohyoidoepiglottopexy).
Total Laryngectomy: (Fig.5 & 6) When the tumour involves a large portion of the larynx, a more aggressive surgery is done to remove entire voice box. This procedure is called total laryngectomy. In order to complete this operation the windpipe must be brought out to the neck to form a permanent opening called stoma. Air can no longer pass from the lungs into the mouth and nose. The inhaled air passes directly through the stoma into the trachea and then into the lungs. The connection between the mouth and oesophagus is usually not affected, so food and liquid can be swallowed just as they were before the operation. As the vocal cords were removed, a laryngectomee patient will no longer have laryngeal speech. This does not mean that speech is lost and there are ways to talk without a larynx.
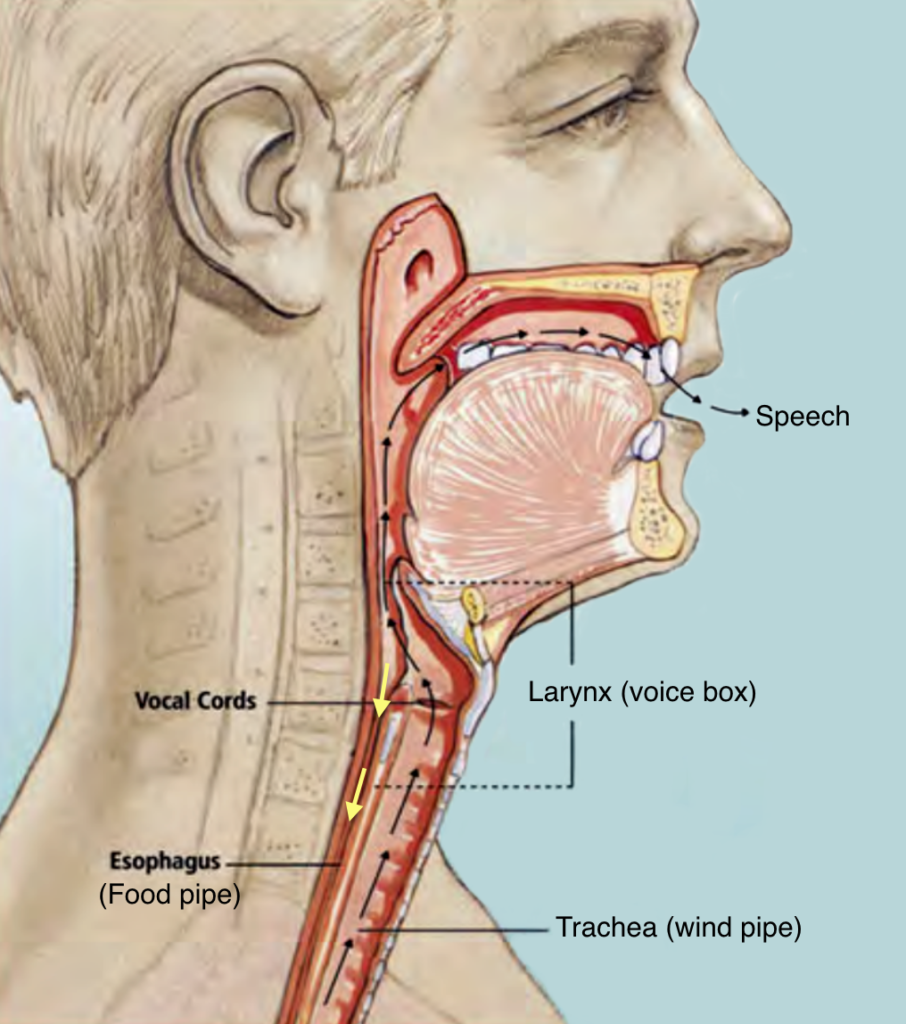
Fig.5. Normal anatomy. Passage for air and food is common upto larynx. The larynx is marked in this picture. Yellow arrow – food passage.
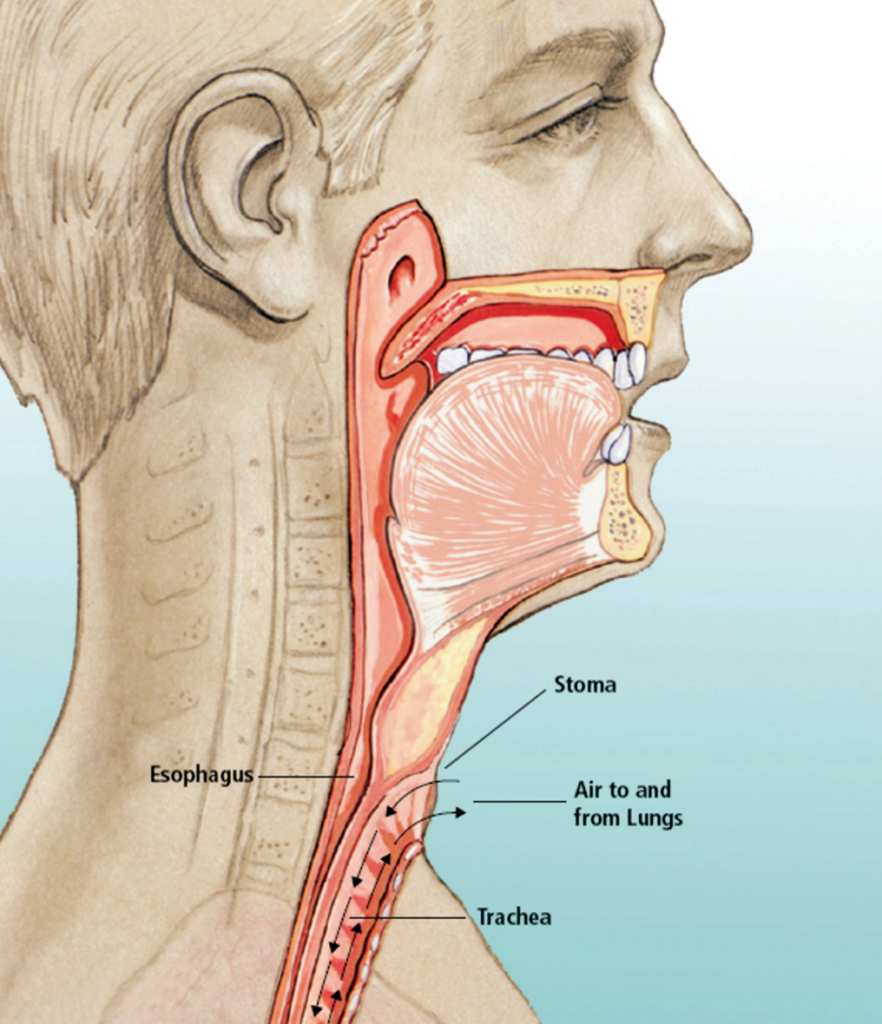
Fig.6. After removal of larynx, the wind pipe (trachea) is stitched to the skin in the lower part of neck. Normal food passage is maintained.
Management of Lymph nodes will be included in whatever treatment plan is felt to be appropriate for the patient. This will involve surgery or radiotherapy. Many times an operation called a neck dissection is done to remove lymph nodes of the neck that may be involved with cancer.
Speech after removal of Larynx (voice box) Alaryngeal Speech:
Even when the patient loses the voice box in total laryngectomy, he/she can still learn to talk. There are basically 3 methods by which patient can learn to talk
Oesophageal Speech: (Fig.7) In this method, patient is taught to swallow the air and then to belch out. When the air comes out, the junction of the pharynx and food pipe acts like vocal cord and with the movement of tongue, palate and lips, speech is produced. The voice will be rough and monotonous. It requires lots of practice and perseverance on the part of the patient. About 50 – 60% of patients develop reasonable speech with this method. Patient has to periodically break the speech to swallow air.
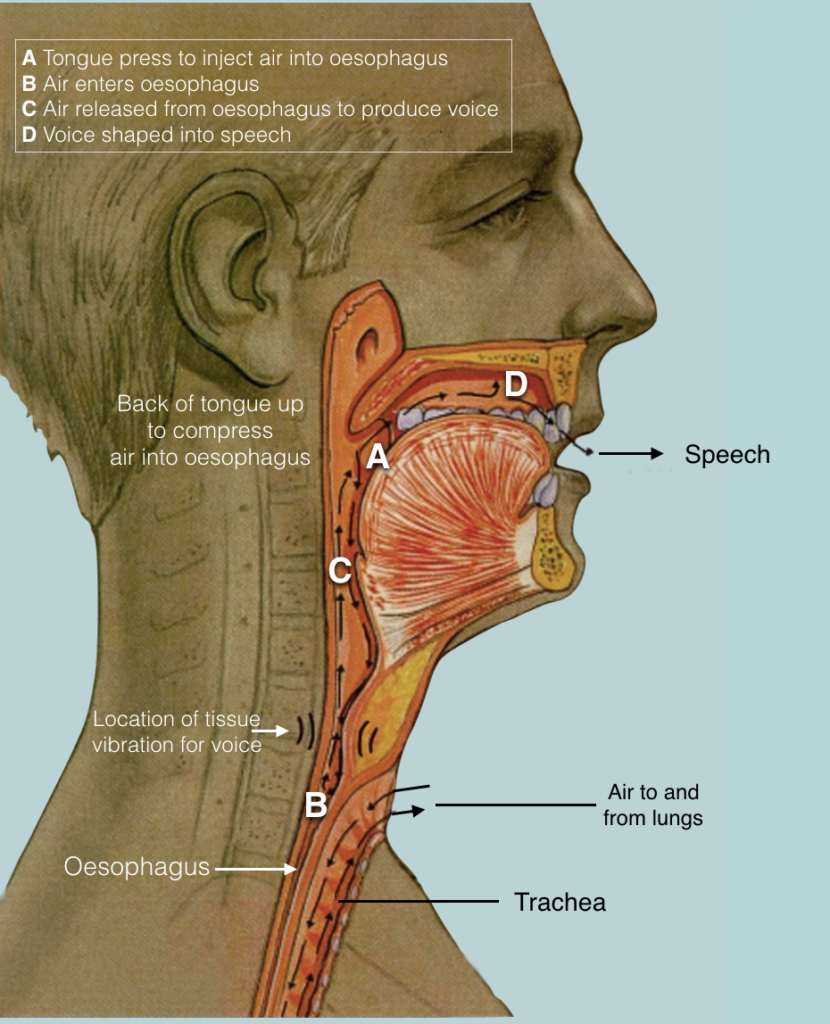
Oesophageal Speech: (Fig.7)
Video – 03 – Oesophageal Speech
In this method, patient is taught to swallow the air and then to belch out. When the air comes out, the junction of the pharynx and food pipe acts like vocal cord and with the movement of tongue, palate and lips, speech is produced. The voice will be rough and monotonous. It requires lots of practice and perseverance on the part of the patient. About 50 – 60% of patients develop reasonable speech with this method. Patient has to periodically break the speech to swallow air.
Electronic Larynx: (Fig.8) It is a hand held electronic device, which has a diaphragm at one end, that vibrates. This end of the device is held over the floor of mouth and the patient start to articulate the tongue and lip musculature. The sounds of these movements are amplified by this device and speech is produced. The speech sounds like robotic speech.
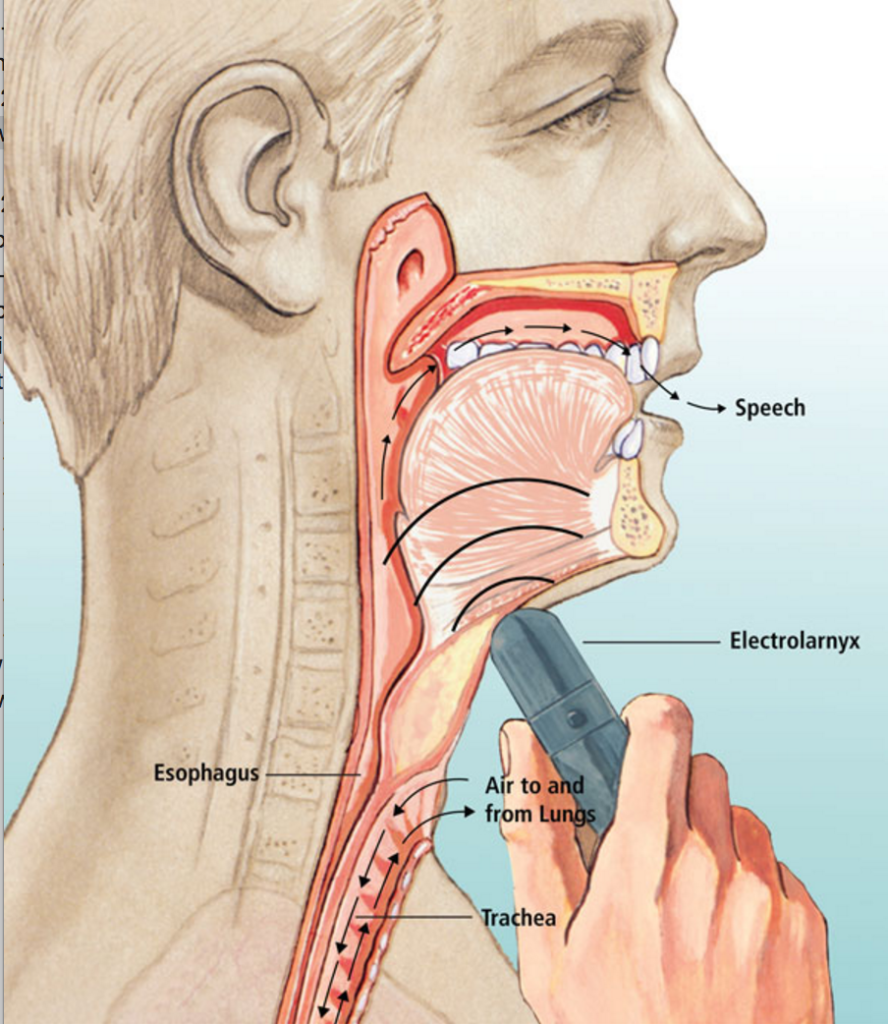
Electronic Larynx: (Fig.8)
Video – 04 – Electrolarynx
Voice Prosthesis: (Fig.9) This device is a valve that is placed surgically between the airway in the neck and the oesophagus (food pipe) (Fig.9). By covering the breathing hole (stoma) in the neck with a finger, a patient is able to force air through the valve into the food pipe (oesophagus) and out of the mouth. Now, we have mechanical valve which closes the stoma when the patient tries to speak and frees the hand. Relatively normal speech is achievable. This valve can be inserted at the time of the cancer surgery itself or later on if the patient does not develop oesophageal speech.
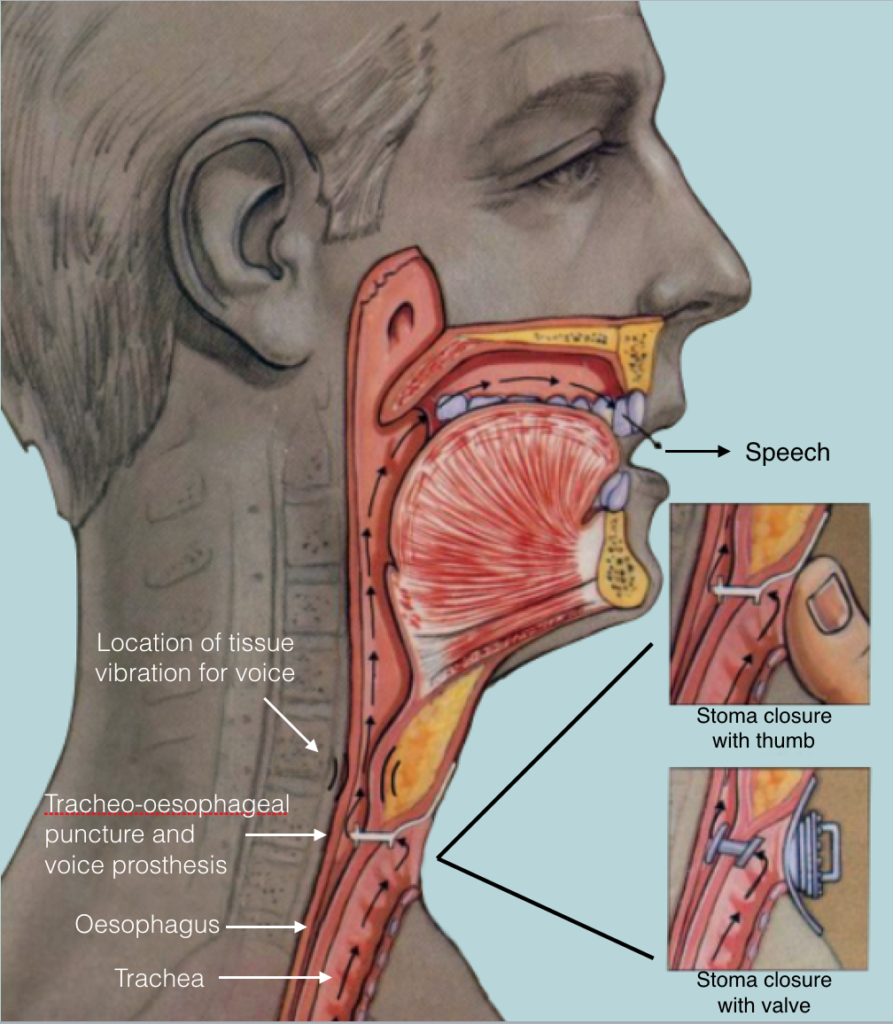
Fig.9. Tracheo-oesophageal puncture and voice prosthesis
Video – 05 – Speech with voice prosthesis
This device is a valve that is placed surgically between the airway in the neck and the oesophagus (food pipe) (Fig.9). By covering the breathing hole (stoma) in the neck with a finger, a patient is able to force air through the valve into the food pipe (oesophagus) and out of the mouth. Now, we have mechanical valve which closes the stoma when the patient tries to speak and frees the hand. Relatively normal speech is achievable. This valve can be inserted at the time of the cancer surgery itself or later on if the patient does not develop oesophageal speech.
Questions patients should ask before deciding about the treatment:
- What are my treatment options?
- What are the risks and benefits for each of my treatment options?
- How will treatment affect my everyday activity? How long?
- How often will I need to return?
- Has my doctor explained various surgical options to my satisfaction?
- Has a surgeon who has expertise with removal of cancer seen me?
- Have I seen by a radiation oncologist?
- Do I know all I need to know about speech rehabilitation techniques?
- How often has the surgeon performed the kind of surgery he is recommending?
- What will the surgical site look like after healing?
- Will my appearance and physical capabilities be affected? If so how?
- Should I consider combination therapy (both surgery and radiation therapy)?
The Heart Of Clinic

Dr. C. Rayappa MBBS, DLO, FRCS(Edin)
SENIOR CONSULTANT
+91 44 3315 1105
Dr. C. Rayappa graduated from Madras Medical College, Chennai, India in 1982. He completed his post graduation in Otolaryngology (ENT)
For Doctors
Need more information?
Reach us through mail or phone
For Patients
Need more information?
Reach us through mail or phone
The Heart Of Clinic
Dr. C. Rayappa MBBS, DLO, FRCS(Edin)
SENIOR CONSULTANT
+91 44 3315 1105
Dr. C. Rayappa graduated from Madras Medical College, Chennai, India in 1982. He completed his post graduation in Otolaryngology (ENT)